

Osteoporotic vertebral endplate and cortex fractures: A pictorial review
- PMID: 30306044
- PMCID: PMC6169255
- DOI: 10.1016/j.jot.2018.08.004
Osteoporotic vertebral endplate and cortex fractures: A pictorial review
Abstract
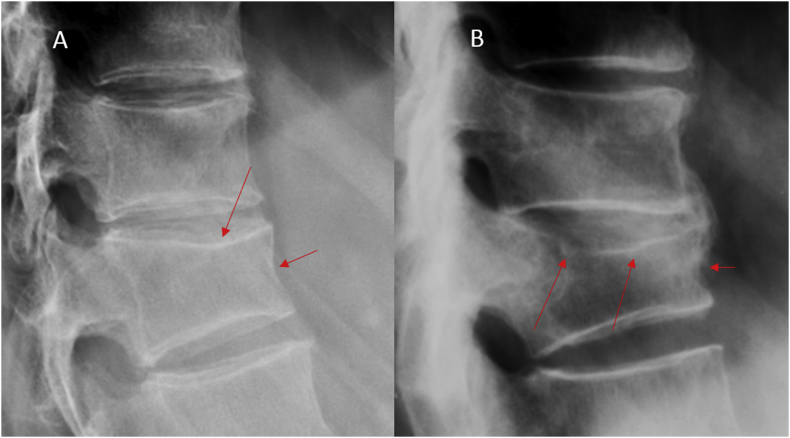
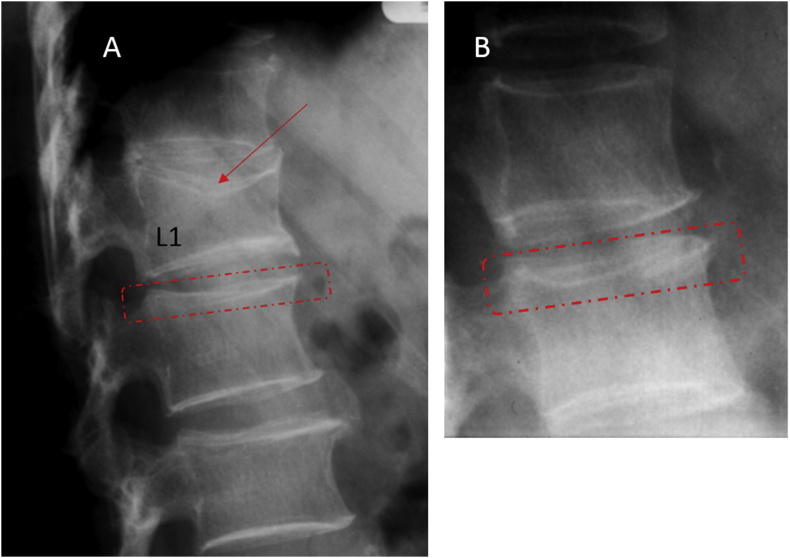
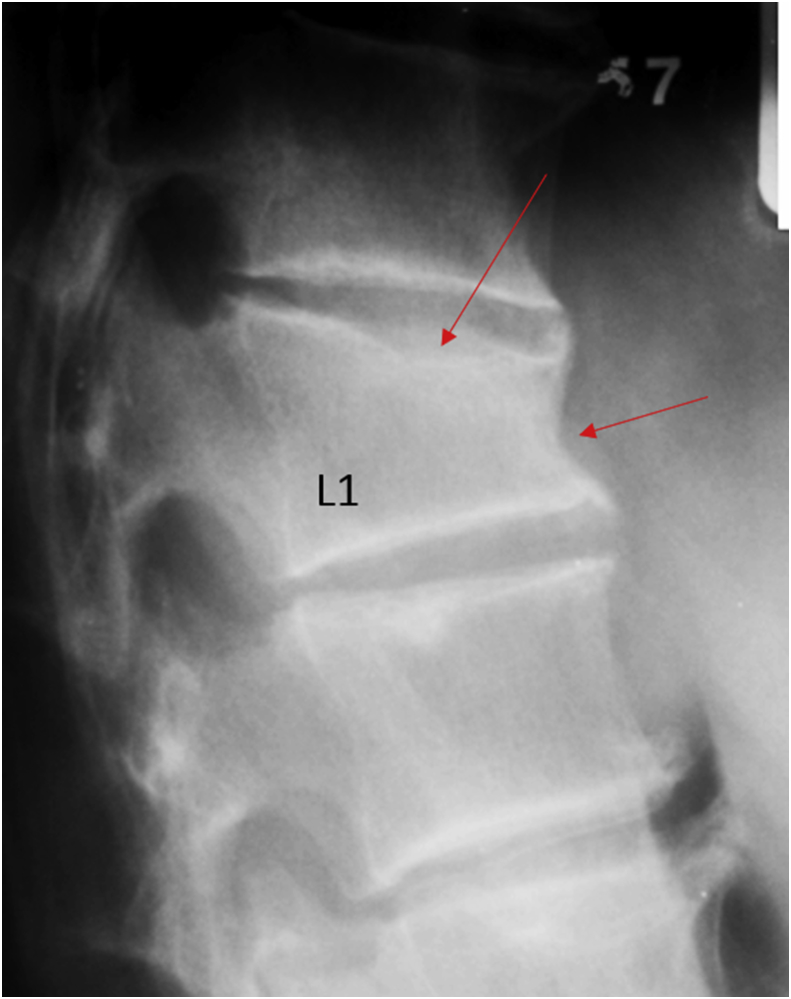
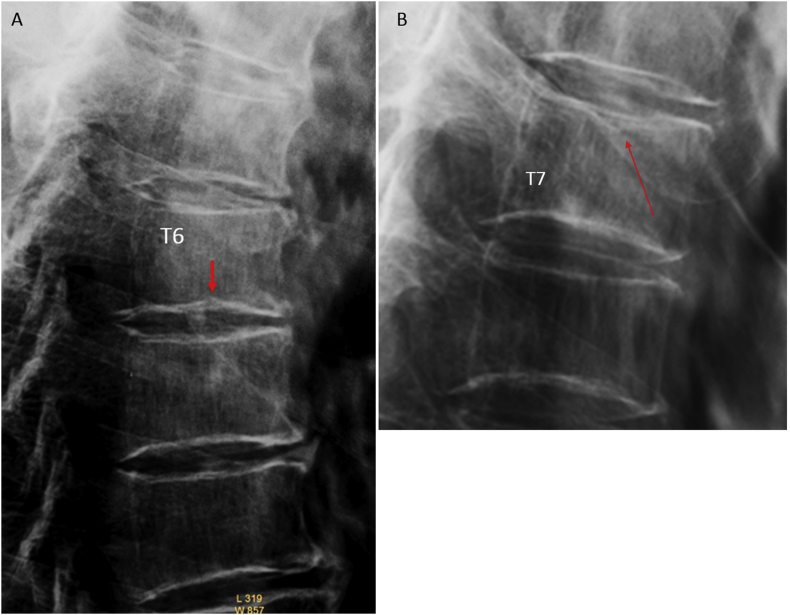
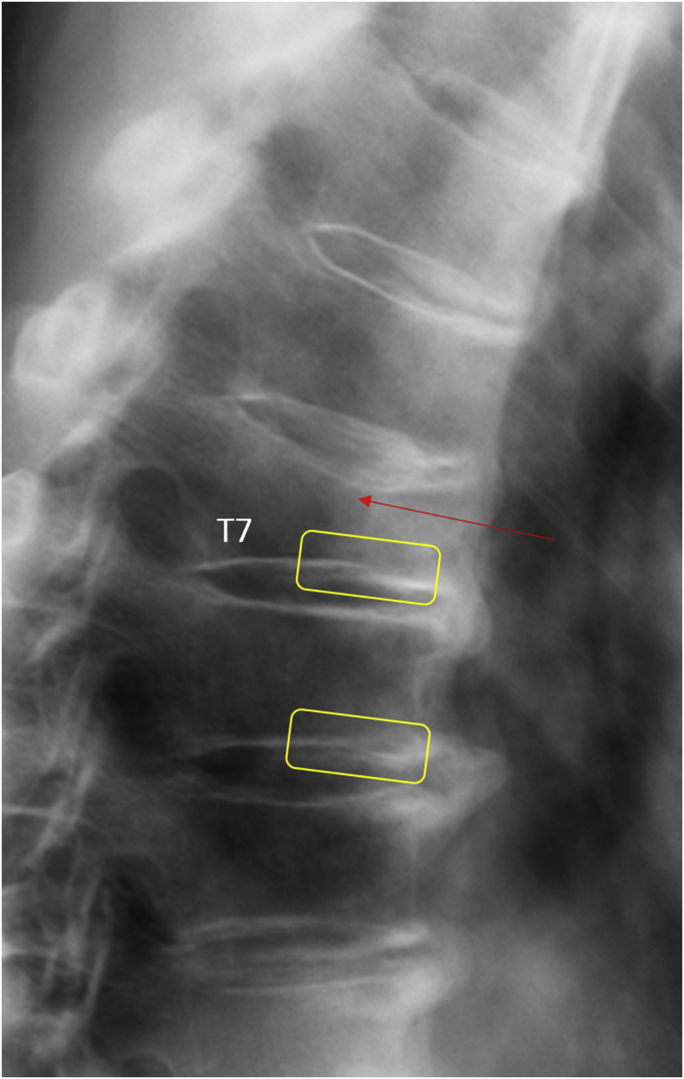
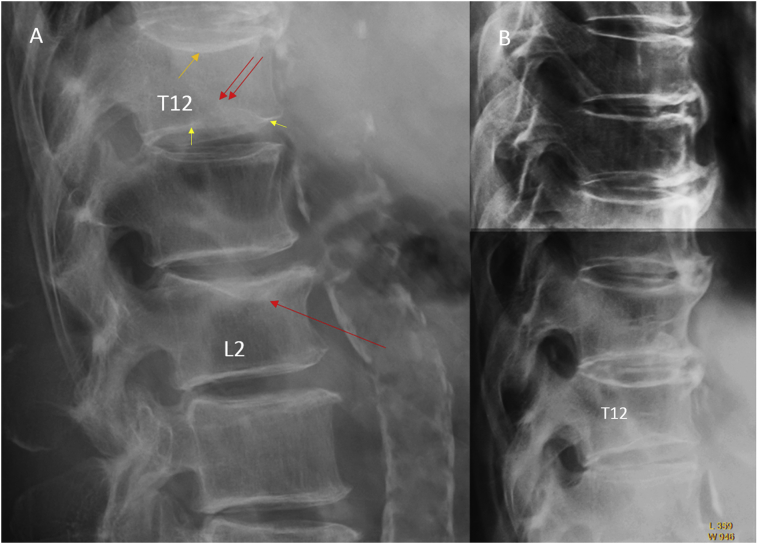
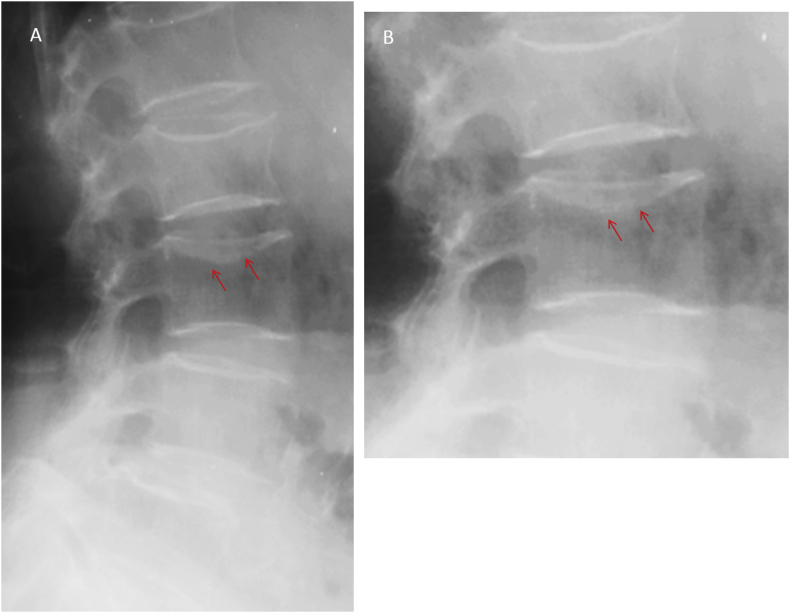
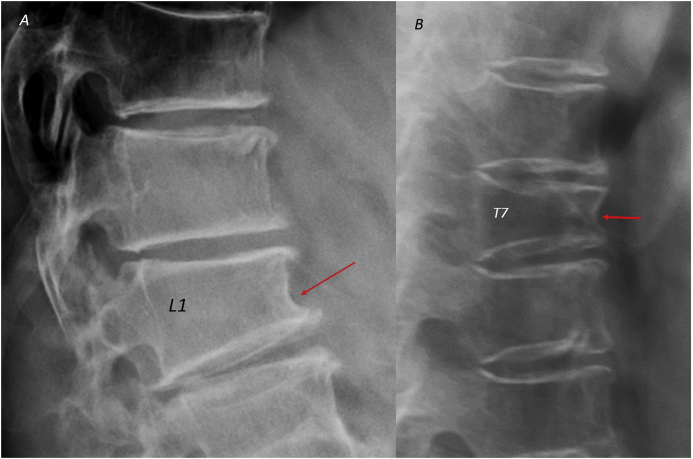
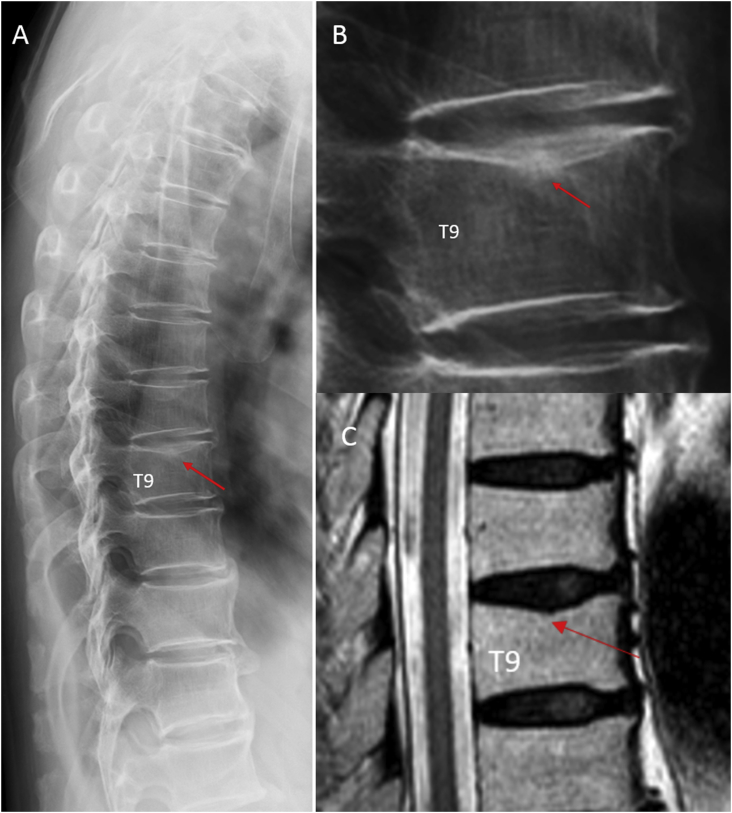
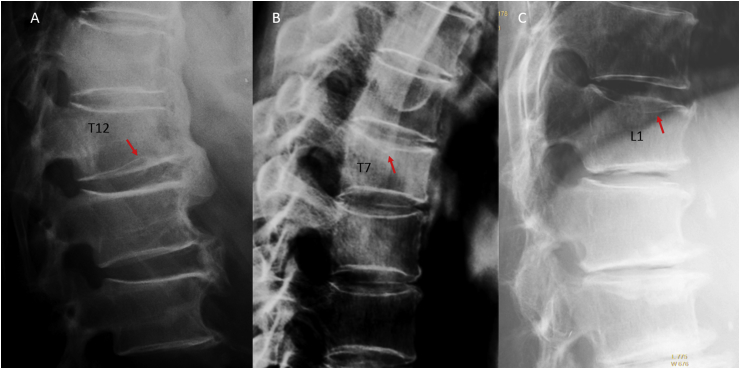
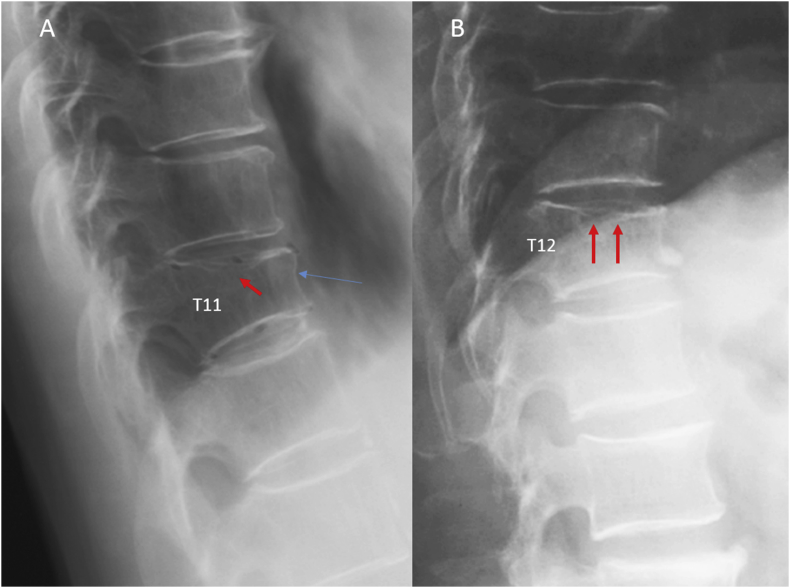
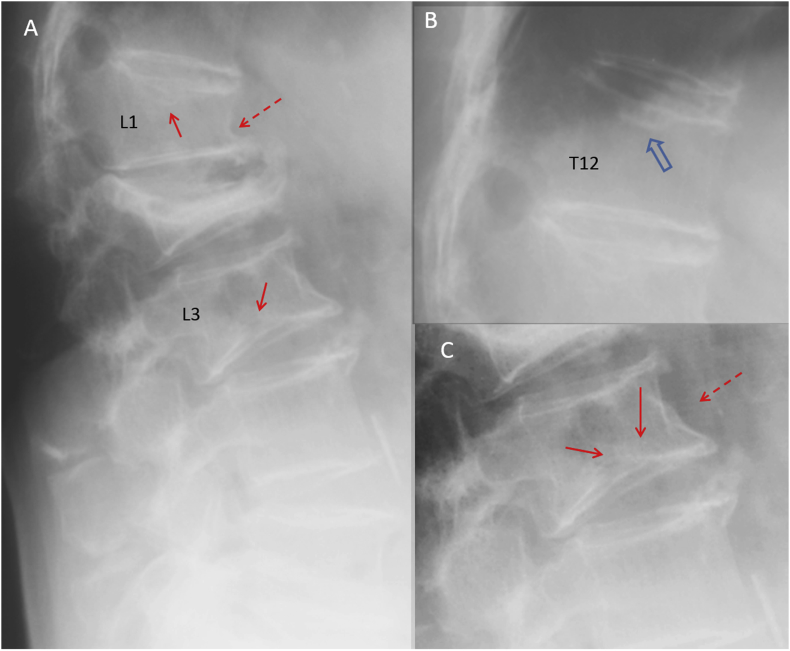
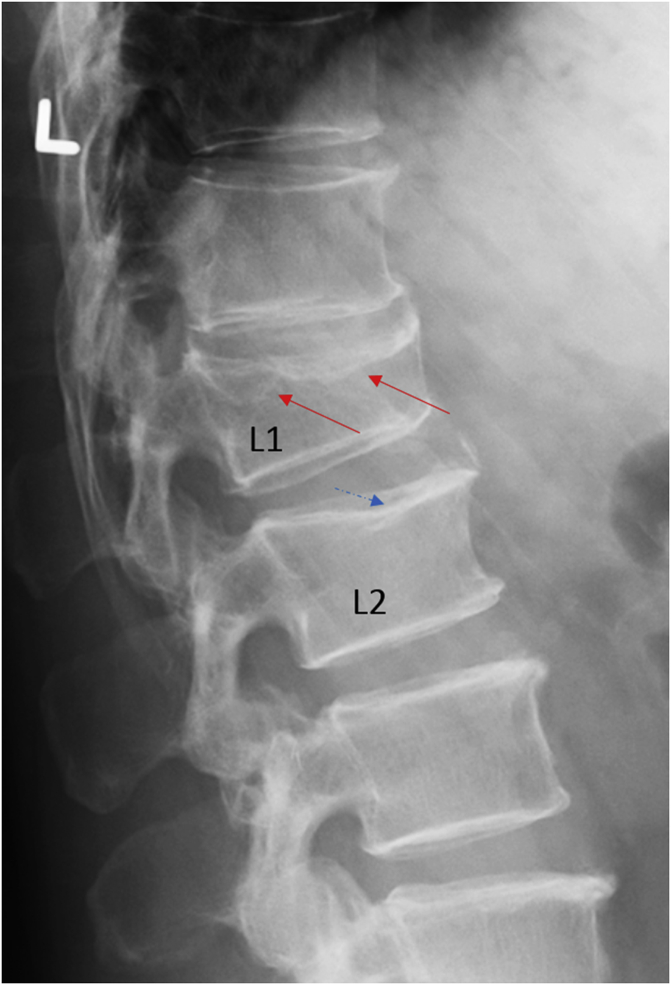
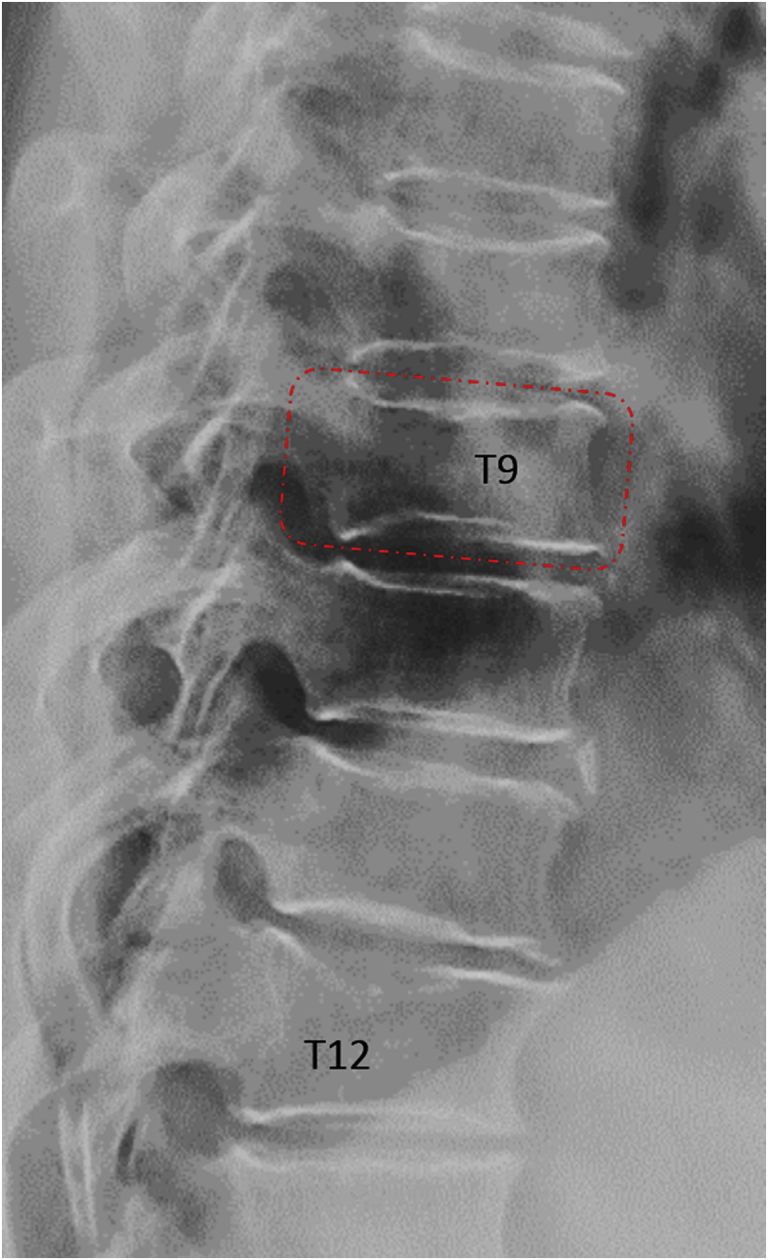
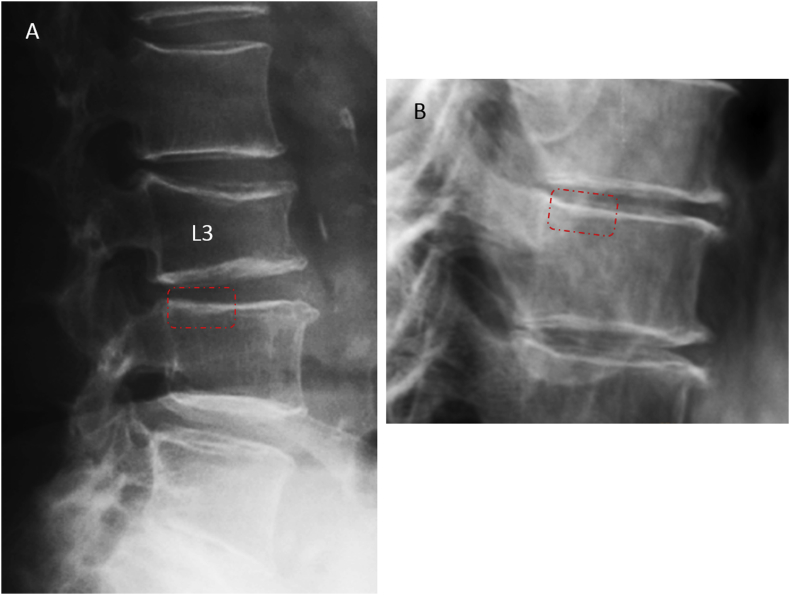
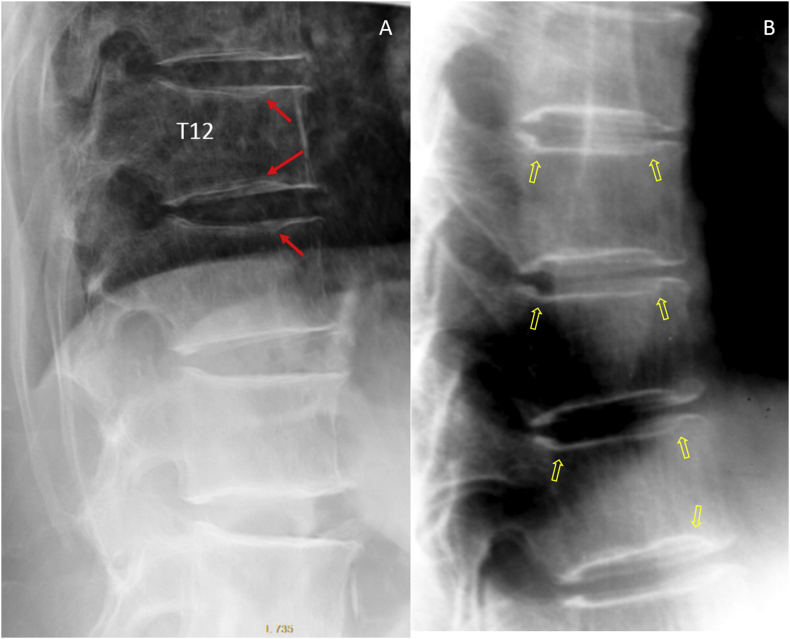
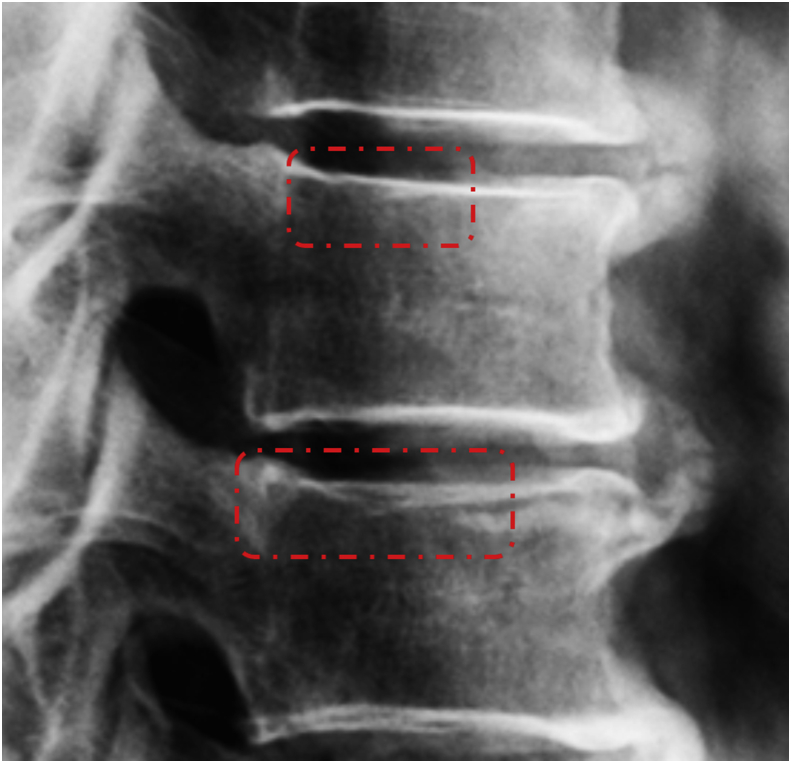
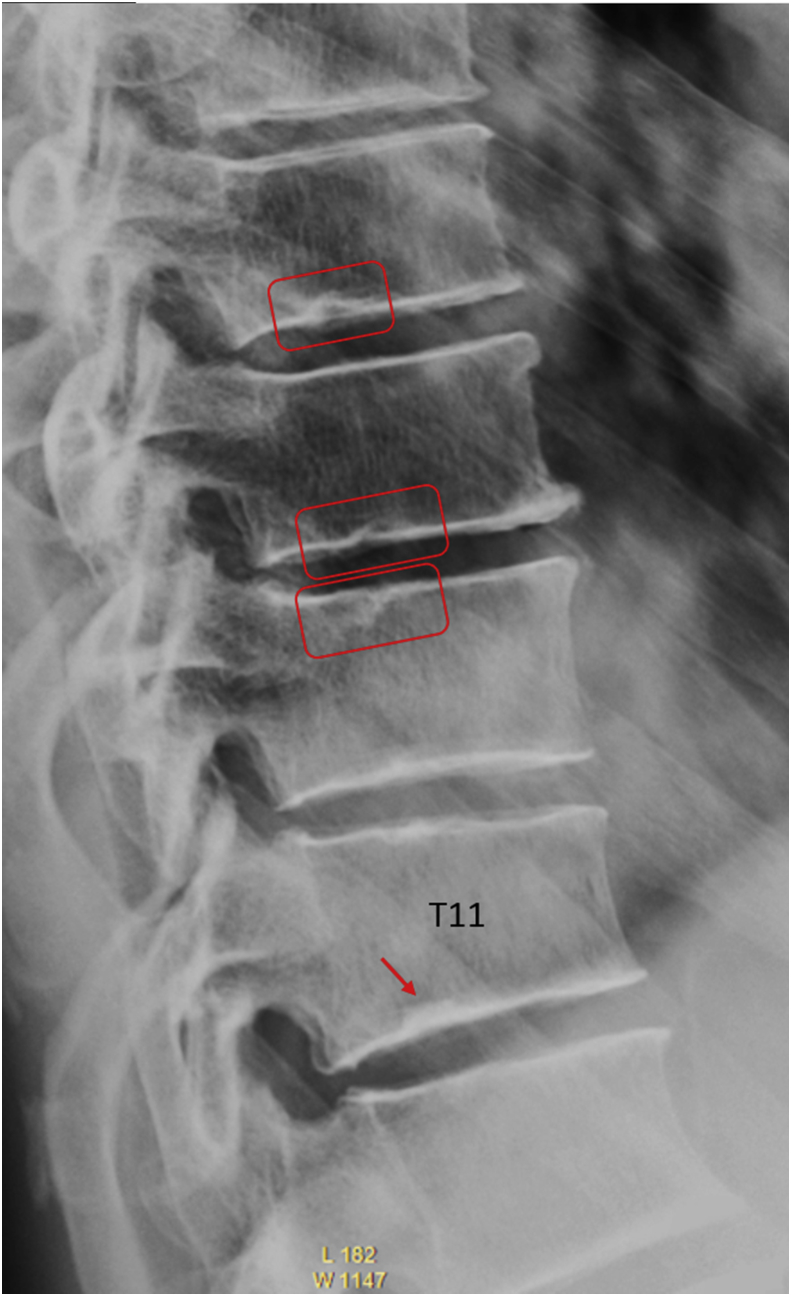
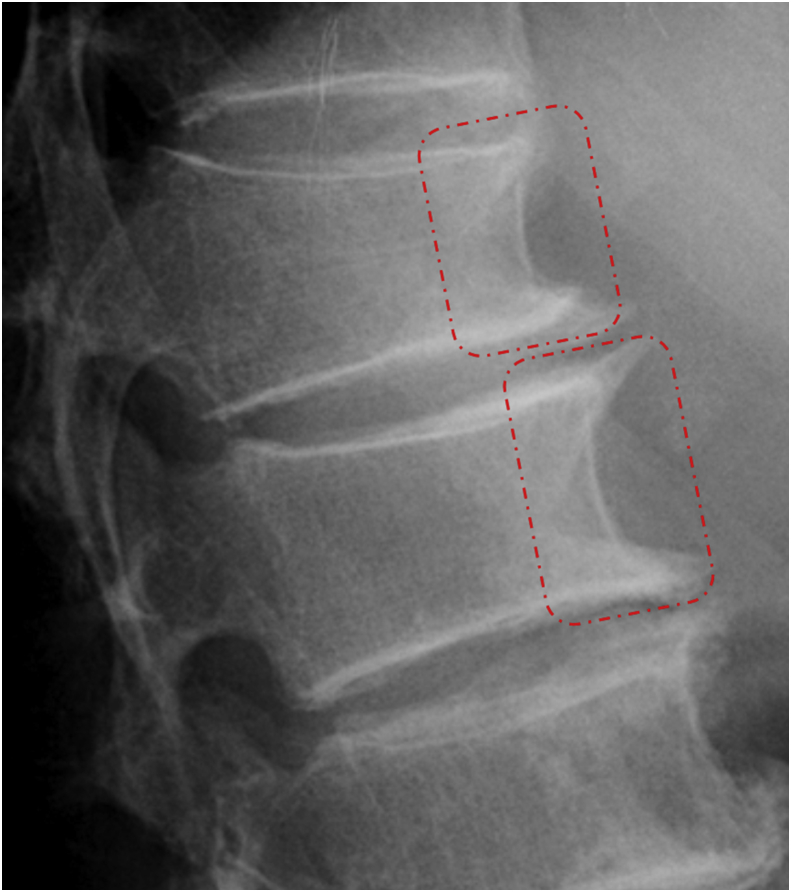
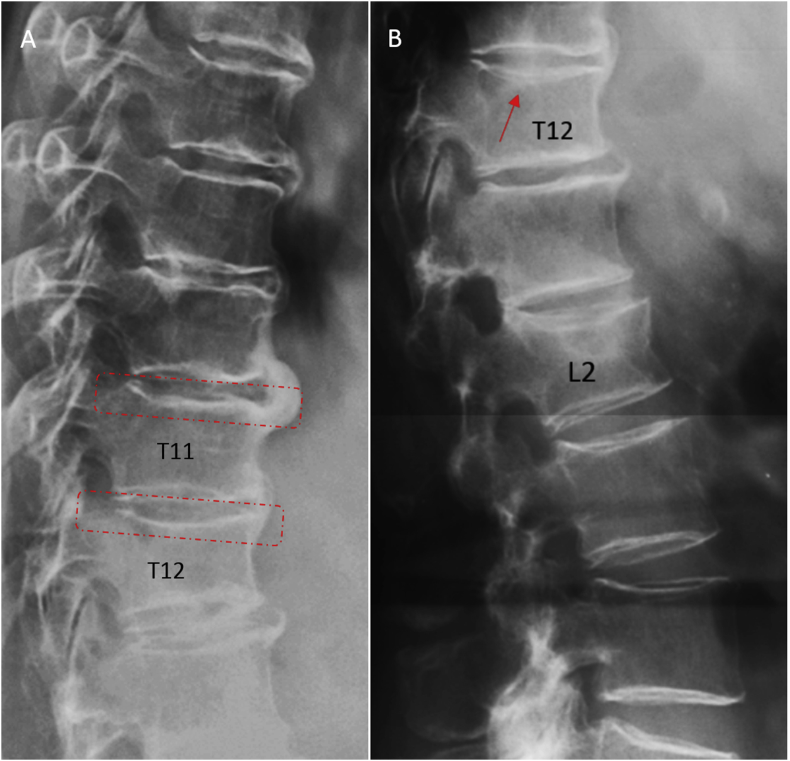
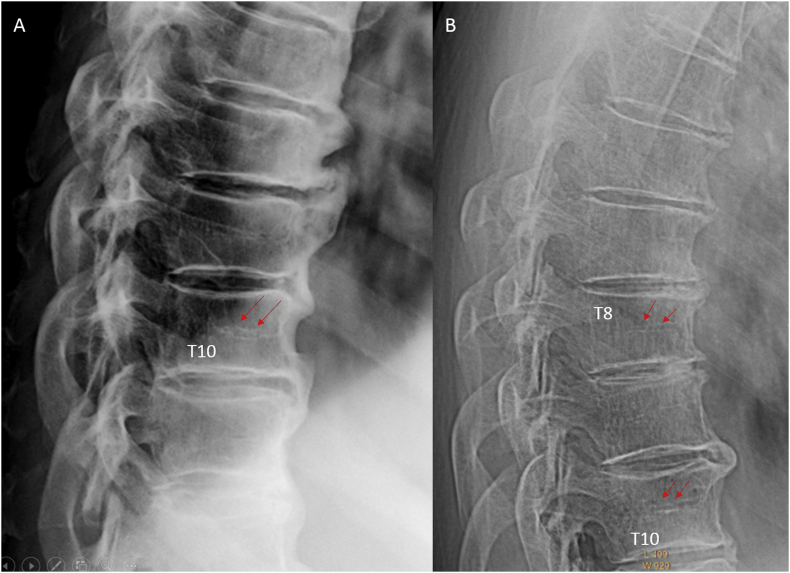
Despite years' research, the radiographic criteria for osteoporotic vertebral fracture and its grading remain debated. The importance of identifying vertebral endplate/cortex fracture (ECF) is being recognised; however, evaluation of osteoporotic ECF requires training and experience. This article aims to serve as a teaching material for radiologists/physicians or researchers to evaluate osteoporotic ECF. Emphasis is particularly dedicated to identifying ECF that may not be associated with apparent vertebral body collapse. We suggest a combined approach based on standardised radiologic evaluation by experts and morphometry measurement is the most appropriate approach to detect and classify osteoporotic vertebral fractures.
The translational potential: A good understanding of radiologic anatomy of vertebrae and fracture signs of endplate/cortex are essential for spine fragility fracture assessment.
Keywords: Endplate; Normal variants; Osteoporosis; Osteoporotic fractures; Radiograph.
Figures




References
-
- Ross P.D. Clinical consequences of vertebral fractures. Am J Med. 1997;103:30S–42S. - PubMed
-
- Kado D.M., Browner W.S., Palermo L., Nevitt M.C., Genant H.K., Cummings S.R. Vertebral fractures and mortality in older women: a prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med. 1999;159:1215–1220. - PubMed
-
- Morin S., Lix L.M., Azimaee M., Metge C., Majumdar S.R., Leslie W.D. Institutionalization following incident non-traumatic fractures in community-dwelling men and women. Osteoporos Int. 2012;23:2381–2386. - PubMed
-
- Cooper C., Atkinson E.J., Jacobsen S.J., O'Fallon W.M., Melton L.J., 3rd Population-based study of survival after osteoporotic fractures. Am J Epidemiol. 1993;137:1001–1005. - PubMed
-
- Nevitt M.C., Ettinger B., Black D.M. The association of radiographically detected vertebral fractures with back pain and function: a prospective study. Ann Intern Med. 1998;128(10):793–800. - PubMed
