

Patterns of the initiation of disease-modifying antirheumatic drugs in incident rheumatoid arthritis: a German perspective based on nationwide ambulatory drug prescription data
- PMID: 30306254
- PMCID: PMC6208685
- DOI: 10.1007/s00296-018-4161-7
Patterns of the initiation of disease-modifying antirheumatic drugs in incident rheumatoid arthritis: a German perspective based on nationwide ambulatory drug prescription data
Abstract
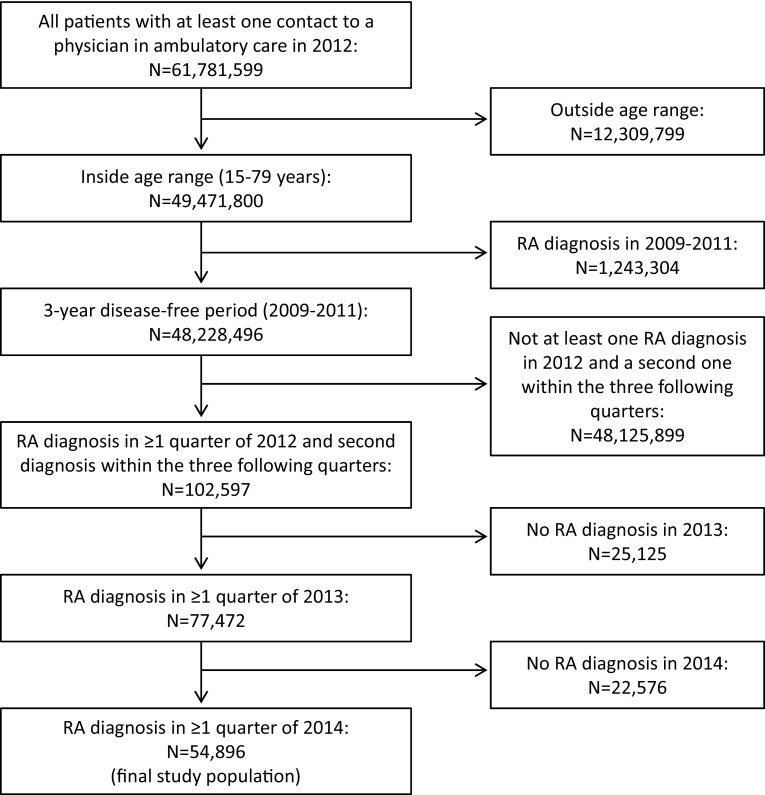
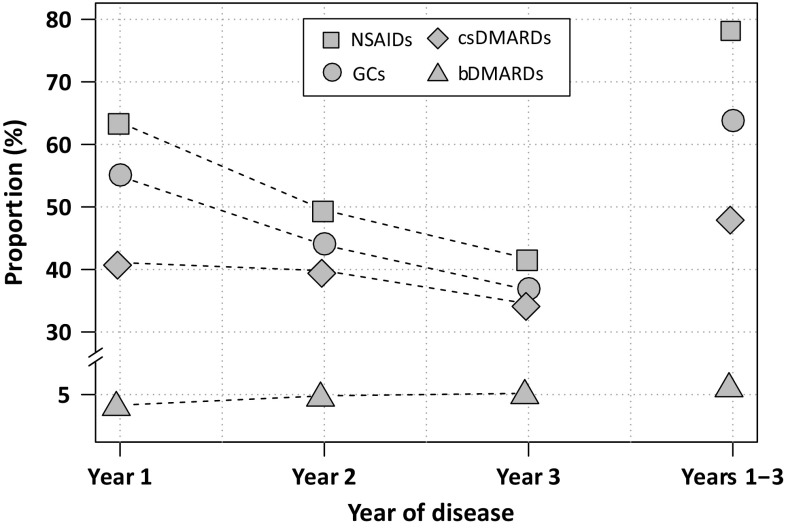
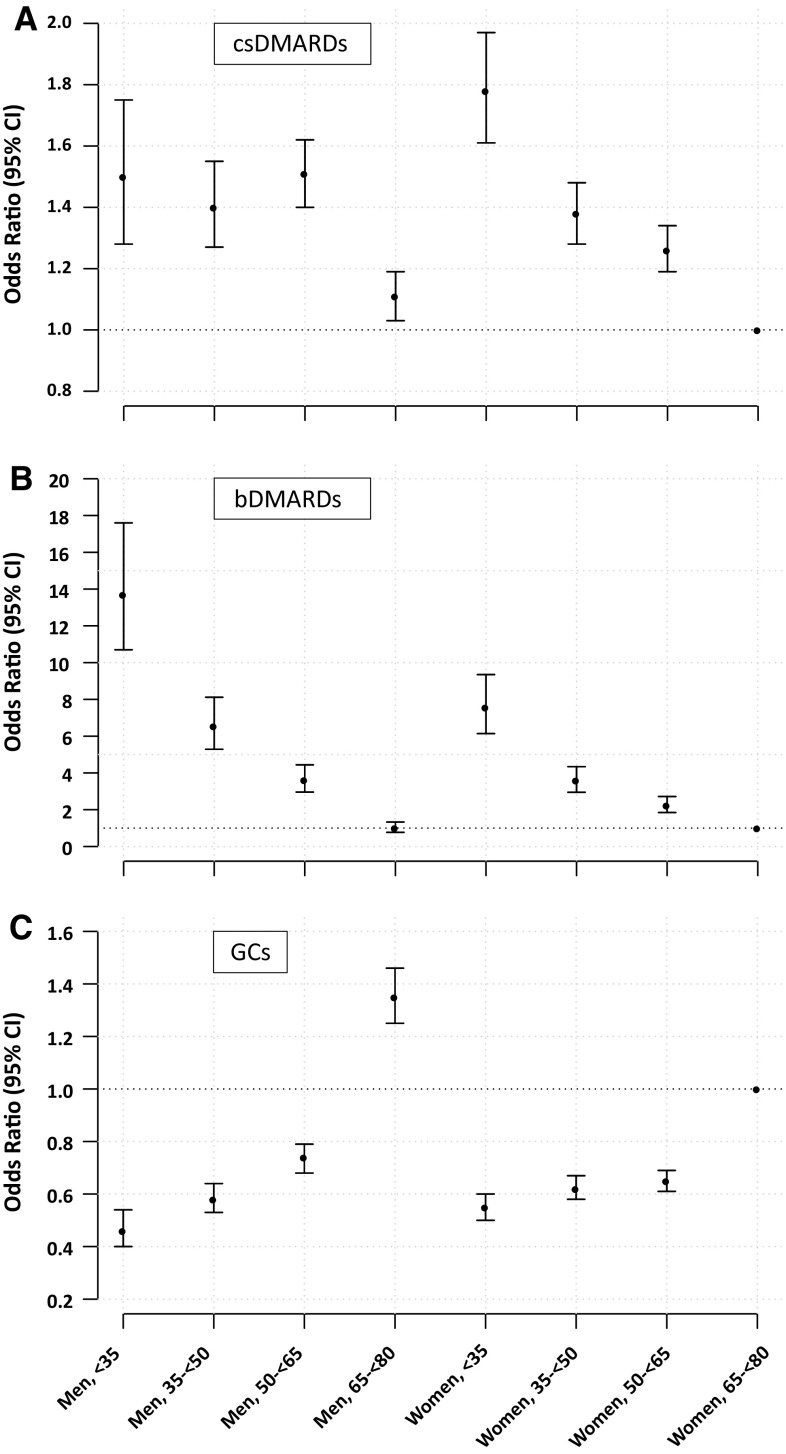
This study aimed at providing a current and nearly complete picture of the patterns of the initiation of disease-modifying antirheumatic drugs (DMARDs) in patients with newly diagnosed RA. Based on ambulatory drug prescription data and physician billing claims data covering 87% of the German population, we assembled a cohort of incident RA patients aged 15-79 years (n = 54,896) and assessed the prescription frequency of total DMARDs, conventional synthetic (csDMARDs) and biologic DMARDs (bDMARDs) within the first year of disease. Using multiple logistic regression, we estimated the chance of early DMARD receipt based on age, sex, serotype and specialty of prescribing physician while controlling for region of residence. In total, 44% of incident RA patients received a DMARD prescription within the first year of disease. In multiple regression, younger patients (< 35 years) had 1.7-fold higher chances of receiving a csDMARD than patients aged ≥ 65 years [odds ratio (OR): 1.65 with 95% confidence interval (CI) 1.51-1.80] and almost tenfold higher chances to receive a bDMARD [OR (95% CI) 9.5 (8.0-11.3)]. Seropositivity and a visit to a rheumatologist were positively associated with DMARD initiation [OR (95% CI) 2.8 (2.6-2.9) and 5.9 (5.6-6.2) for csDMARDs, respectively]. Based on data covering 87% of the German population, the present study revealed that less than half of incident RA patients receive DMARDs within the first year of disease and that marked differences exist according to age. The study highlights the importance of involving a rheumatologist early in the management of RA.
Keywords: Ambulatory drug prescription data; Biologicals; Disease-modifying antirheumatic drugs; Glucocorticoids; Non-steroidal anti-inflammatory drugs; Rheumatoid arthritis.
Conflict of interest statement
Conflict of interest
AS declares that she has no conflict of interest. JH declares that he has no conflict of interest. KK declares that she has no conflict of interest. MKA declares that he has no conflict of interest. JB declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. This study was exempted from institutional review board oversight and informed consent since only anonymized data were analysed in accordance with § 300 paragraph 2 Volume V of the Social Security Code (Sozialgesetzbuch (SGB) V).
Figures
References
-
- Gibofsky A. Overview of epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis. Am J Manag Care. 2012;18(13 Suppl):S295–S302. - PubMed
-
- Steffen A, Holstiege J, Goffrier B, Bätzing J (2017) Epidemiology of rheumatoid arthritis in Germany—an analysis based on nationwide claims data of outpatient care. Central Research Institute of Ambulatory Health Care in Germany. https://www.versorgungsatlas.de/fileadmin/ziva_docs/85/VA-85-Rheumatoide.... Accessed 20 Apr 2018
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
