

Estimation of sodium and chloride storage in critically ill patients: a balance study
- PMID: 30306364
- PMCID: PMC6179979
- DOI: 10.1186/s13613-018-0442-2
Estimation of sodium and chloride storage in critically ill patients: a balance study
Abstract
Background: Nonosmotic sodium storage has been reported in animals, healthy individuals and patients with hypertension, hyperaldosteronism and end-stage kidney disease. Sodium storage has not been studied in ICU patients, who frequently receive large amounts of sodium chloride-containing fluids. The objective of our study was to estimate sodium that cannot be accounted for by balance studies in critically ill patients. Chloride was also studied. We used multiple scenarios and assumptions for estimating sodium and chloride balances.
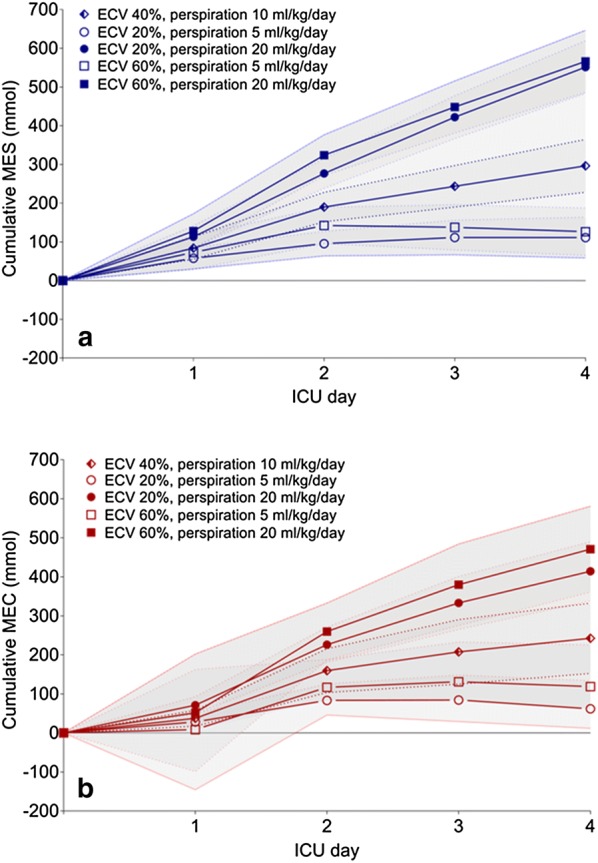
Methods: We retrospectively analyzed patients admitted to the ICU after cardiothoracic surgery with complete fluid, sodium and chloride balance data for the first 4 days of ICU treatment. Balances were obtained from meticulously recorded data on intake and output. Missing extracellular osmotically active sodium (MES) was calculated by subtracting the expected change in plasma sodium from the observed change in plasma sodium derived from balance data. The same method was used to calculate missing chloride (MEC). To address considerable uncertainties on the estimated extracellular volume (ECV) and perspiration rate, various scenarios were used in which the size of the ECV and perspiration were varied.
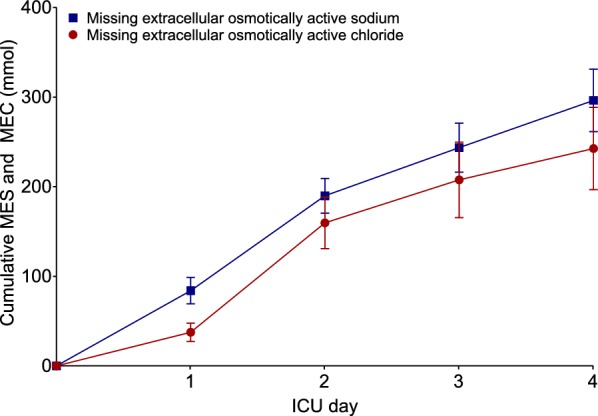
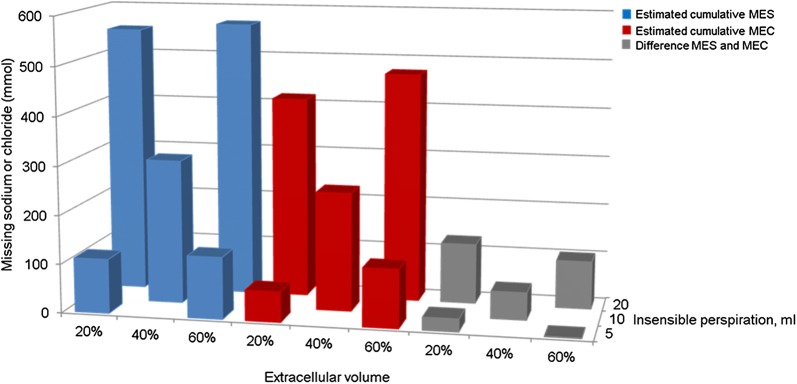
Results: A total of 38 patients with 152 consecutive ICU days were analyzed. In our default scenario, we could not account for 296 ± 35 mmol of MES in the first four ICU days. The range of observed MES in the five scenarios varied from 111 ± 27 to 566 ± 41 mmol (P < 0.001). A cumulative value of 243 ± 46 mmol was calculated for MEC in the default scenario. The range of cumulative MEC was between 62 ± 27 and 471 ± 56 mmol (P = 0.001 and P = 0.003). MES minus MEC varied from 1 ± 51 to 123 ± 33 mmol in the five scenarios.
Conclusions: Our study suggests considerable disappearance of osmotically active sodium in critically ill patients and is the first to also suggest rather similar disappearance of chloride from the extracellular space. Various scenarios for insensible water loss and estimated size for the ECV resulted in considerable MES and MEC, although these estimates showed a large variation. The mechanisms and the tissue compartments responsible for this phenomenon require further investigation.
Keywords: Chloride; Extracellular volume; Intensive care unit; Intracellular volume; Sodium.
Figures
References
-
- Linz P, Santoro D, Renz W, Rieger J, Ruehle A, Ruff J, et al. Skin sodium measured with 23Na MRI at 7.0 T. NMR Biomed. 2015;28:54–62. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
