

Role of imaging in the routine management of endometrial cancer
- PMID: 30306593
- PMCID: PMC6636928
- DOI: 10.1002/ijgo.12618
Role of imaging in the routine management of endometrial cancer
Abstract
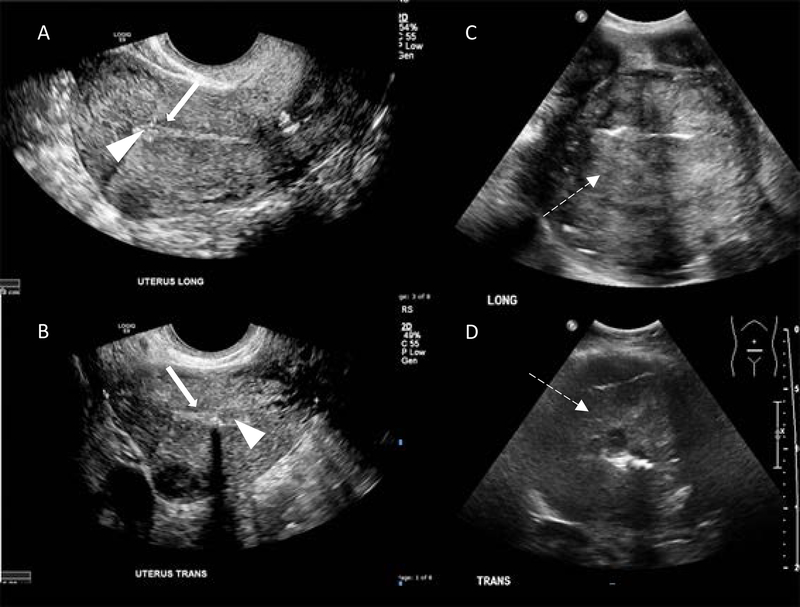
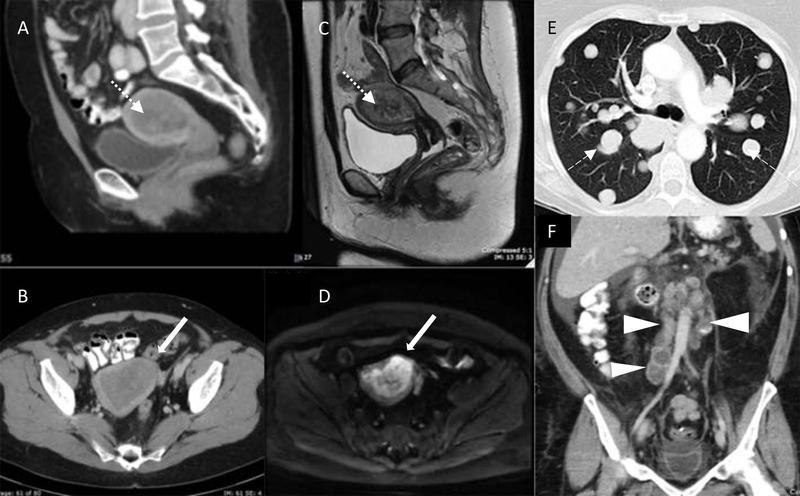
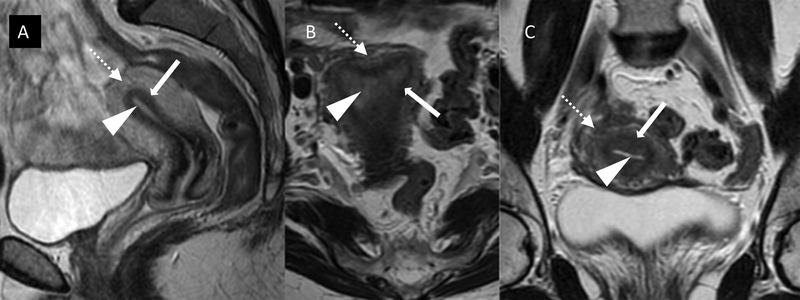
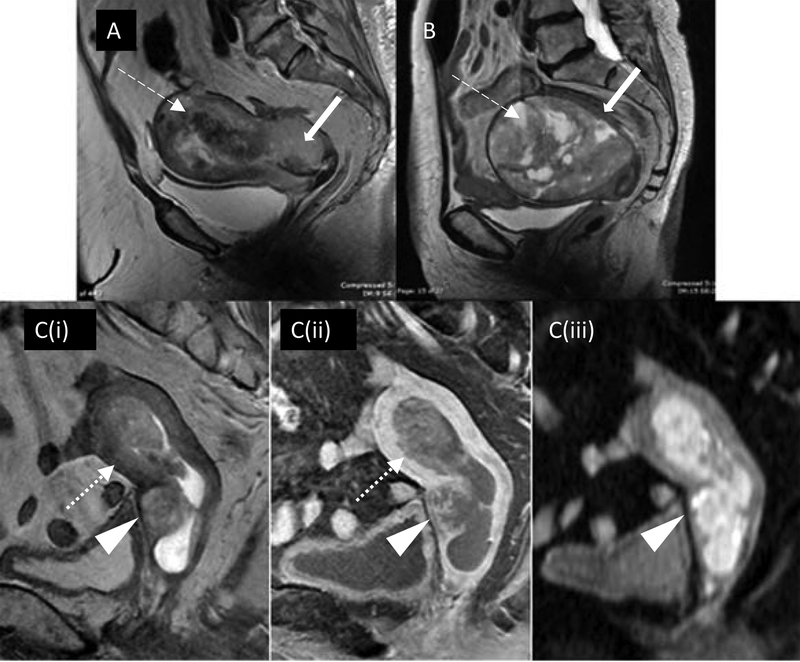
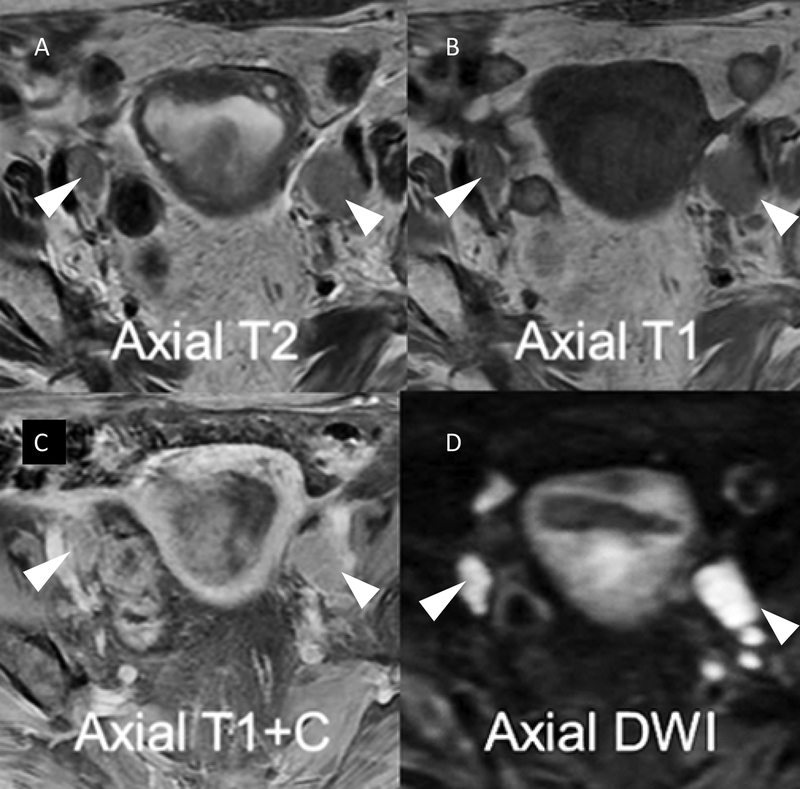
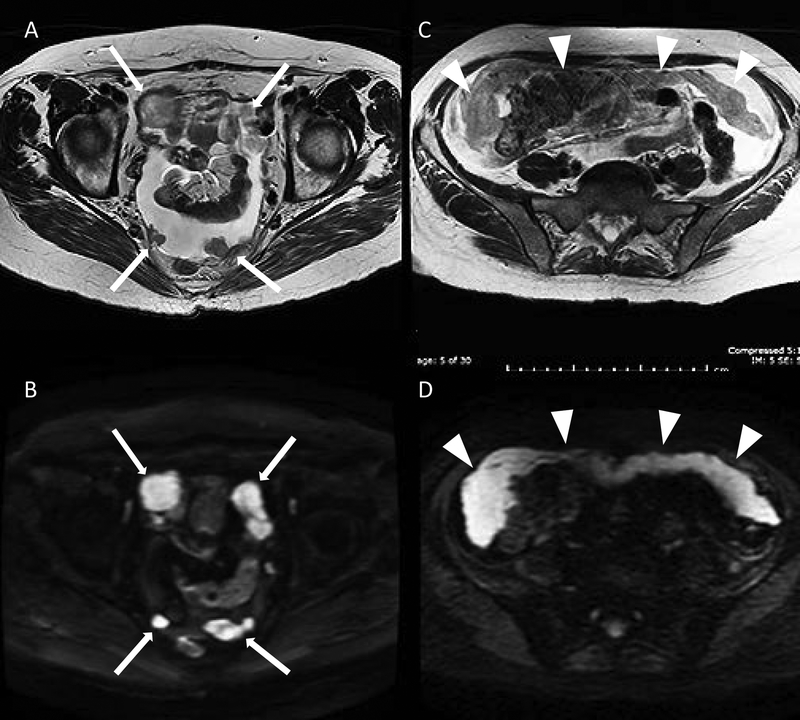
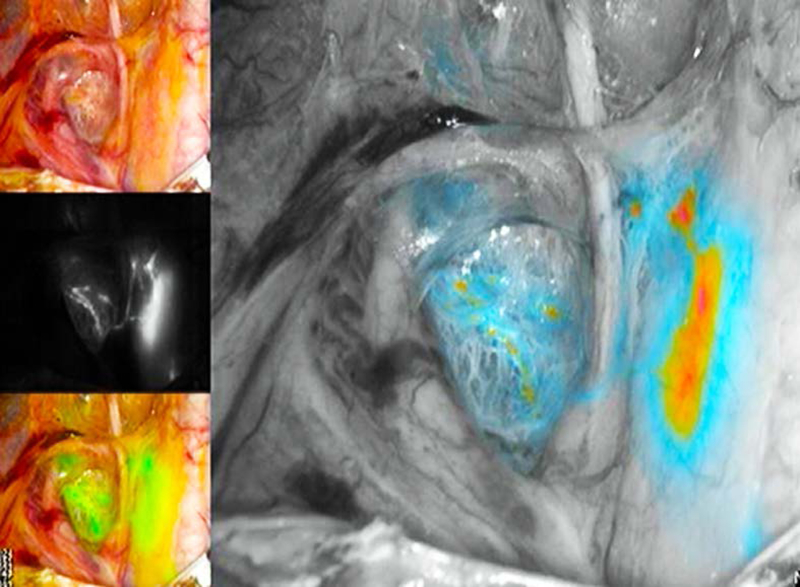
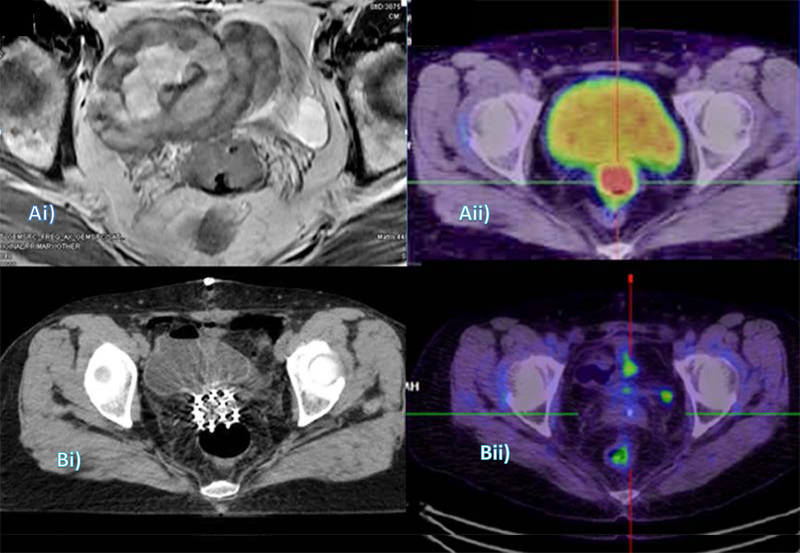
Endometrial cancer is the most common gynecologic cancer in women today. It is surgically staged, and while surgery is the primary treatment modality, the identification of disease extent-in particular extrauterine spread-prior to surgery is important to optimize treatment decision making. Ultrasound and MRI are useful for evaluating the extent of local disease, while CT and PET are used for detecting lymph node or distant metastases. Diffusion-weighted MRI has also been used for detecting small metastatic deposits in lymph nodes and omentum. Extrauterine soft tissue involvement can be detected by ultrasound, CT, MRI, and PET. Recently, intraoperative visualization techniques, such as sentinel lymph node mapping, are increasingly used to avoid extensive surgical staging without compromising treatment. Imaging is also used for planning adjuvant treatment and detection of postoperative residual disease in high-risk patients, monitoring and detecting recurrent disease, and in post-treatment surveillance of asymptomatic patients with high risk of relapse.
Keywords: Endometrial cancer; FIGO Cancer Report; MRI; PET; Radiology; Ultrasound.
© 2018 The Authors. International Journal of Gynecology & Obstetrics published by John Wiley & Sons Ltd on behalf of International Federation of Gynecology and Obstetrics.
Conflict of interest statement
Conflict of interest
The authors have no conflicts of interest to declare.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018;68(1):7–30. - PubMed
-
- Dijkhuizen FP, Mol BW, Brolmann HA, Heintz AP. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia: a meta-analysis. Cancer 2000;89:1765–1772. - PubMed
-
- Abdaal A, Mushtaq Y, Khasati L, Moneim J, Khan F, Ahmed H, et al. Post-menopausal bleeding - Is transvaginal ultrasound a useful first-line investigation in tamoxifen users? Post Reprod Health 2018:2053369118755190. - PubMed
-
- Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer 1987;60(8 Suppl):2035–2041. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
