

Development and validation of a nomogram to predict recurrence and melanoma-specific mortality in patients with negative sentinel lymph nodes
- PMID: 30307046
- PMCID: PMC6585628
- DOI: 10.1002/bjs.10995
Development and validation of a nomogram to predict recurrence and melanoma-specific mortality in patients with negative sentinel lymph nodes
Abstract
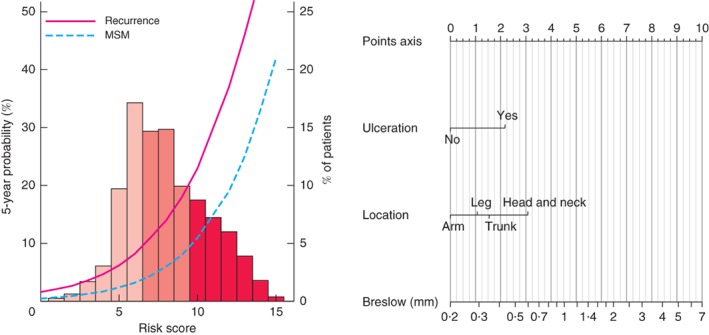
Background: Patients with melanoma and negative sentinel nodes (SNs) have varying outcomes, dependent on several prognostic factors. Considering all these factors in a prediction model might aid in identifying patients who could benefit from a personalized treatment strategy. The objective was to construct and validate a nomogram for recurrence and melanoma-specific mortality (MSM) in patients with melanoma and negative SNs.
Methods: A total of 3220 patients with negative SNs were identified from a cohort of 4124 patients from four EORTC Melanoma Group centres who underwent sentinel lymph node biopsy. Prognostic factors for recurrence and MSM were studied with Cox regression analysis. Significant factors were incorporated in the models. Performance was assessed by discrimination (c-index) and calibration in cross-validation across the four centres. A nomogram was developed for graphical presentation.
Results: There were 3180 eligible patients. The final prediction model for recurrence and the calibrated model for MSM included three independent prognostic factors: ulceration, anatomical location and Breslow thickness. The c-index was 0·74 for recurrence and 0·76 for the calibrated MSM model. Cross-validation across the four centres showed reasonable model performance. A nomogram was developed based on these models. One-third of the patients had a 5-year recurrence probability of 8·2 per cent or less, and one-third had a recurrence probability of 23·0 per cent or more.
Conclusion: A nomogram for predicting recurrence and MSM in patients with melanoma and negative SNs was constructed and validated. It could provide personalized estimates useful for tailoring surveillance strategies (reduce or increase intensity), and selection of patients for adjuvant therapy or clinical trials.
© 2018 The Authors. BJS published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
References
-
- Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK et al Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992; 127: 392–399. - PubMed
-
- Balch CM, Soong SJ, Gershenwald JE, Thompson JF, Reintgen DS, Cascinelli N et al Prognostic factors analysis of 17 600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J Clin Oncol 2001; 19: 3622–3634. - PubMed
-
- Leiter U, Stadler R, Mauch C, Hohenberger W, Brockmeyer N, Berking C et al Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG‐SLT): a multicentre, randomised, phase 3 trial. Lancet Oncol 2016; 17: 757–767. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
