

Performances of five risk algorithms in predicting cardiovascular events in patients with Psoriatic Arthritis: An Italian bicentric study
- PMID: 30308025
- PMCID: PMC6181379
- DOI: 10.1371/journal.pone.0205506
Performances of five risk algorithms in predicting cardiovascular events in patients with Psoriatic Arthritis: An Italian bicentric study
Abstract
Introduction: In patients with psoriatic arthritis (PsA) an increased cardiovascular (CV) risk has been observed. Recently, a EULAR taskforce suggested to use a multiplication by the factor of 1.5 of CV risk algorithms in patients with inflammatory arthritis. This study aims to evaluate the performance of five original and adapted according to EULAR recommendations CV risk algorithms in PsA: SCORE, CUORE, Framingham Risk Score (FRS), QRISK2, and Reynold's Risk Score (RRS).
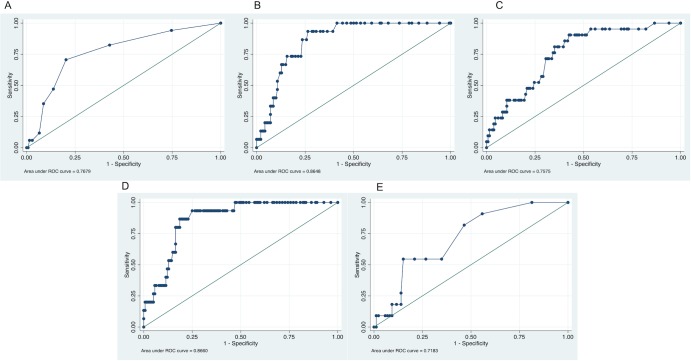
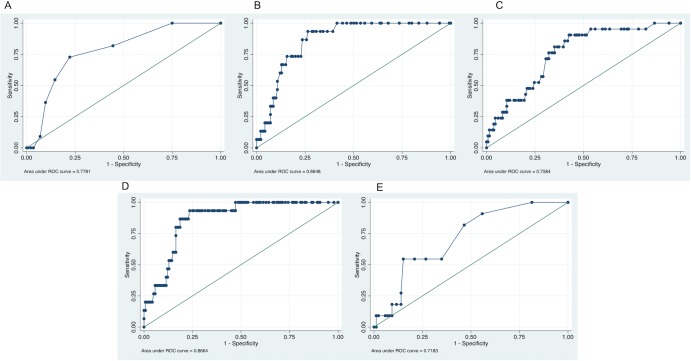
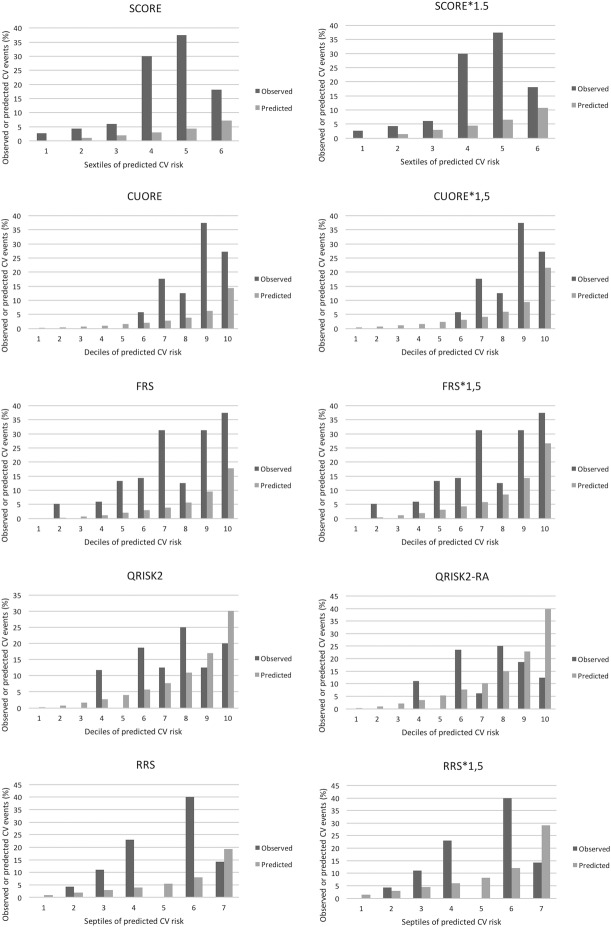
Methods: Prospectively collected data from two Italian cohorts were used. Discriminatory ability for CV risk prediction was evaluated by the area under the ROC curves. Calibration between predicted and observed events was assessed by Hosmer-Lemeshow (HL) tests. Sensibility and specificity were calculated for low-to-intermediate and intermediate-to-high risk cut-offs.
Results: One hundred fifty-five patients were enrolled with an observation of 1550 patient/years. Area under the ROC were 0.7679 (95% CI 0.64768 to 0.88812), 0.864 (95% CI 0.79675 to 0.93278), 0.7575 (95% CI 0.65784 to 0.85708), 0.8660 (95% CI 0.79428 to 0.93772), and 0.7183 (95% CI 0.57795 to 0.85862) for SCORE, CUORE, FRS, QRSIK2, and RRS, respectively. HL tests demonstrated poor model fit (p<0.05) for SCORE, CUORE, and RRS. Discriminative ability and calibration were not improved by adaption of the algorithms according to EULAR recommendations. Up to 80% of CV events occurred in patients at "low risk" and up to 93% of CV events in patients at "low-intermediate risk".
Conclusions: Adaption of the CV risk algorithms according to EULAR indications did not provide improvement in discriminative ability and calibration in patients with PsA.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Costa L, Caso F, D'Elia L, Atteno M, Peluso R, Del Puente A, et al. Psoriatic arthritis is associated with increased arterial stiffness in the absence of known cardiovascular risk factors: a case control study. Clinical rheumatology. 2012;31(4):711–5. Epub 2011/11/25. 10.1007/s10067-011-1892-1 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
