

Oral iron exacerbates colitis and influences the intestinal microbiome
- PMID: 30308045
- PMCID: PMC6181268
- DOI: 10.1371/journal.pone.0202460
Oral iron exacerbates colitis and influences the intestinal microbiome
Abstract
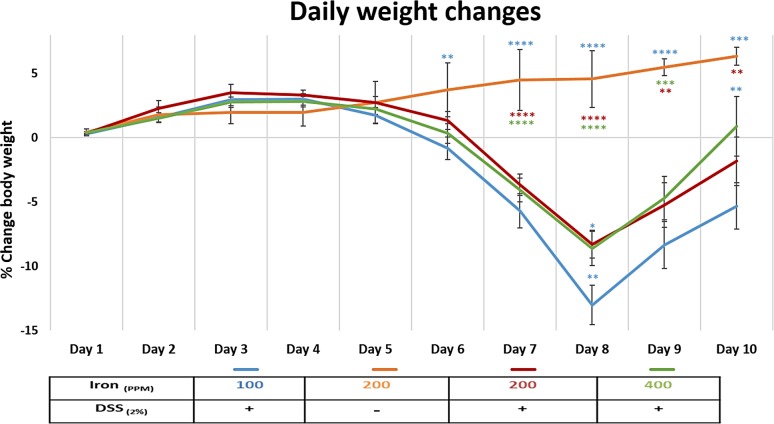
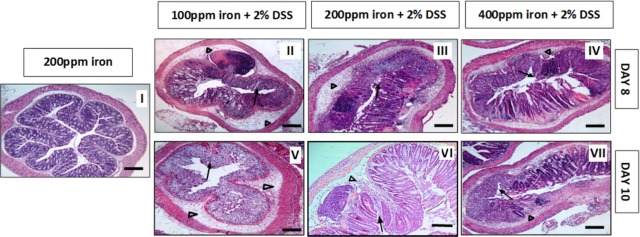
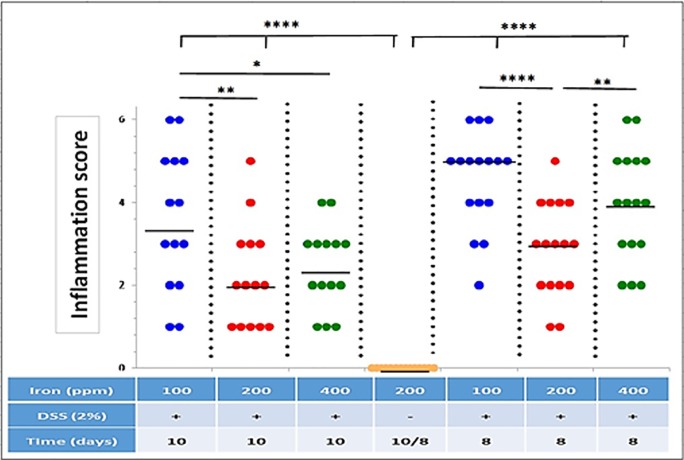
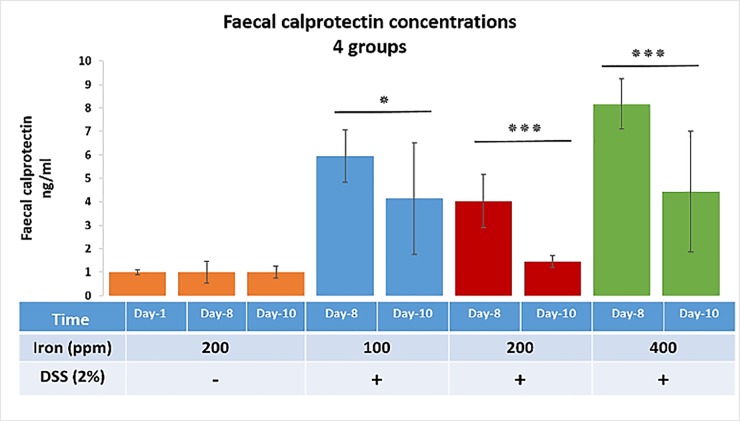
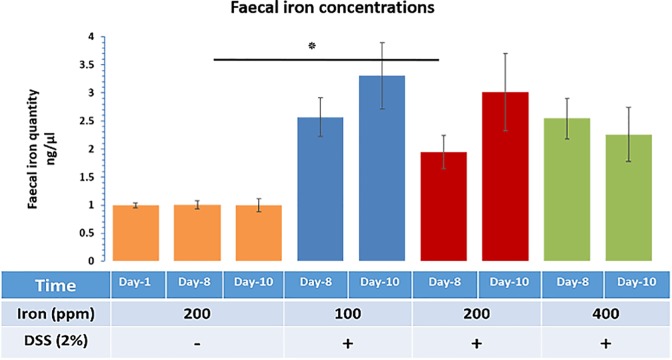
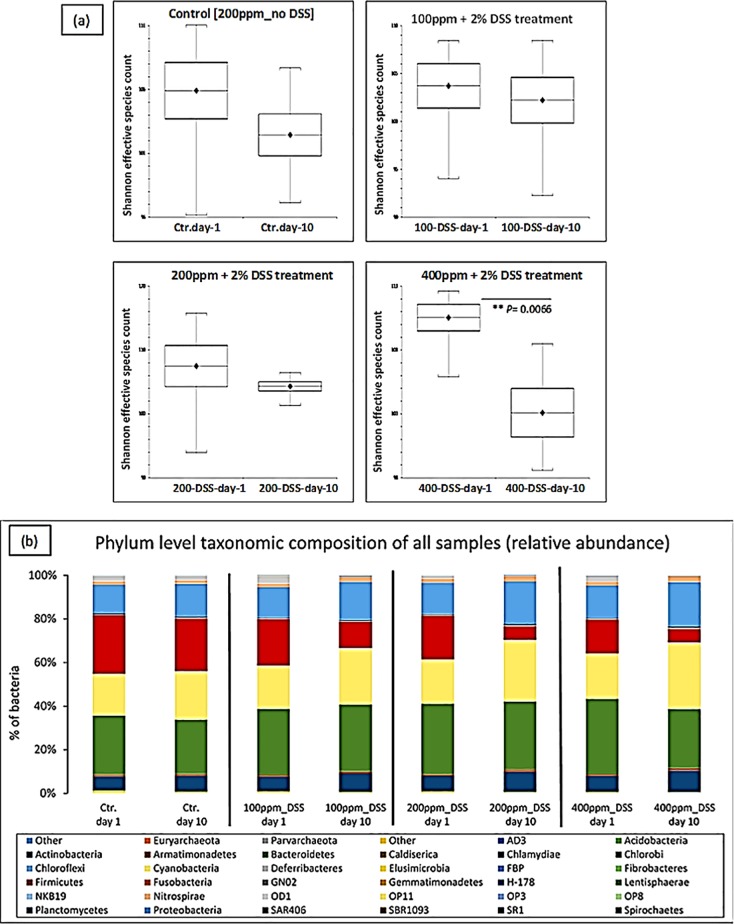
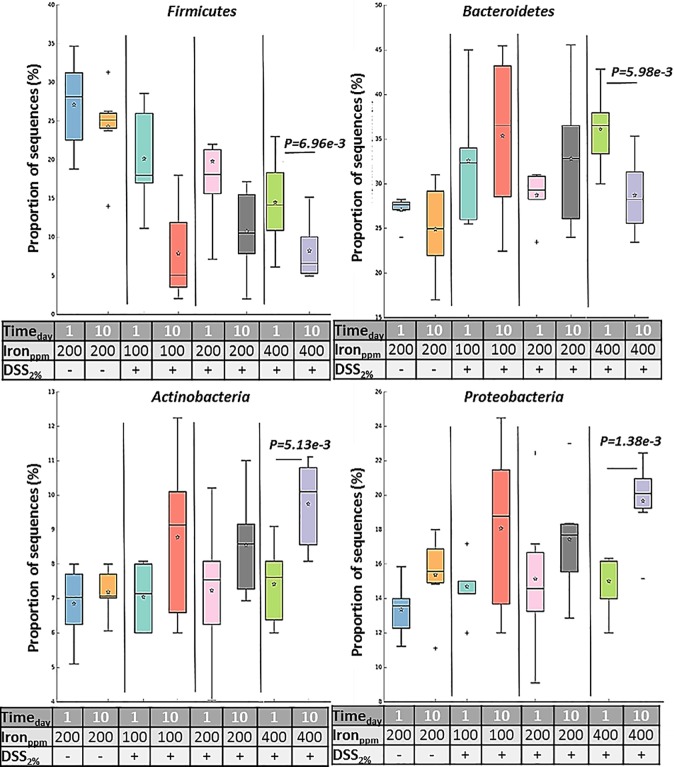
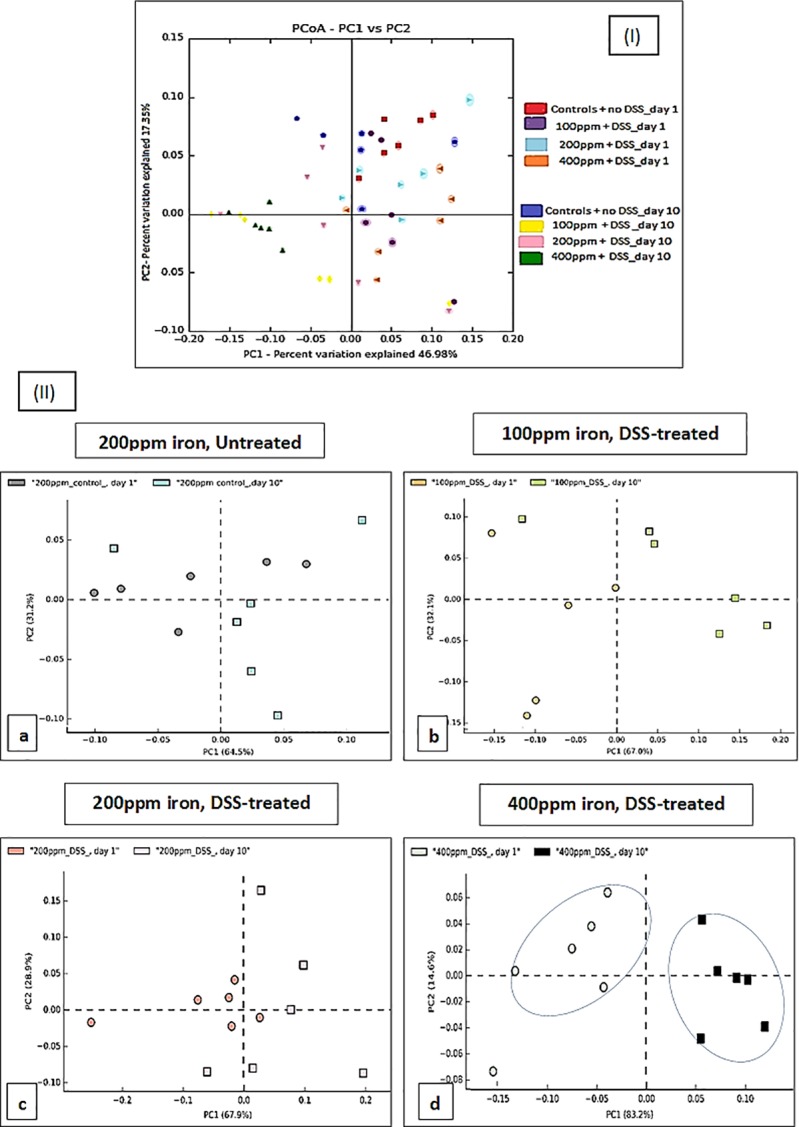
Inflammatory bowel disease (IBD) is associated with anaemia and oral iron replacement to correct this can be problematic, intensifying inflammation and tissue damage. The intestinal microbiota also plays a key role in the pathogenesis of IBD, and iron supplementation likely influences gut bacterial diversity in patients with IBD. Here, we assessed the impact of dietary iron, using chow diets containing either 100, 200 or 400 ppm, fed ad libitum to adult female C57BL/6 mice in the presence or absence of colitis induced using dextran sulfate sodium (DSS), on (i) clinical and histological severity of acute DSS-induced colitis, and (ii) faecal microbial diversity, as assessed by sequencing the V4 region of 16S rRNA. Increasing or decreasing dietary iron concentration from the standard 200 ppm exacerbated both clinical and histological severity of DSS-induced colitis. DSS-treated mice provided only half the standard levels of iron ad libitum (i.e. chow containing 100 ppm iron) lost more body weight than those receiving double the amount of standard iron (i.e. 400 ppm); p<0.01. Faecal calprotectin levels were significantly increased in the presence of colitis in those consuming 100 ppm iron at day 8 (5.94-fold) versus day-10 group (4.14-fold) (p<0.05), and for the 400 ppm day-8 group (8.17-fold) versus day-10 group (4.44-fold) (p<0.001). In the presence of colitis, dietary iron at 400 ppm resulted in a significant reduction in faecal abundance of Firmicutes and Bacteroidetes, and increase of Proteobacteria, changes which were not observed with lower dietary intake of iron at 100 ppm. Overall, altering dietary iron intake exacerbated DSS-induced colitis; increasing the iron content of the diet also led to changes in intestinal bacteria diversity and composition after colitis was induced with DSS.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Manfred Wick WP, Paul Lehmann. Clinical Aspects and Laboratory–Iron Metabolism. 6th ed. SpingerWienNewYork: Springer Vienna; 2011.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
