

Modeling a rotator cuff tear: Individualized shoulder muscle forces influence glenohumeral joint contact force predictions
- PMID: 30308434
- PMCID: PMC6252115
- DOI: 10.1016/j.clinbiomech.2018.10.004
Modeling a rotator cuff tear: Individualized shoulder muscle forces influence glenohumeral joint contact force predictions
Abstract
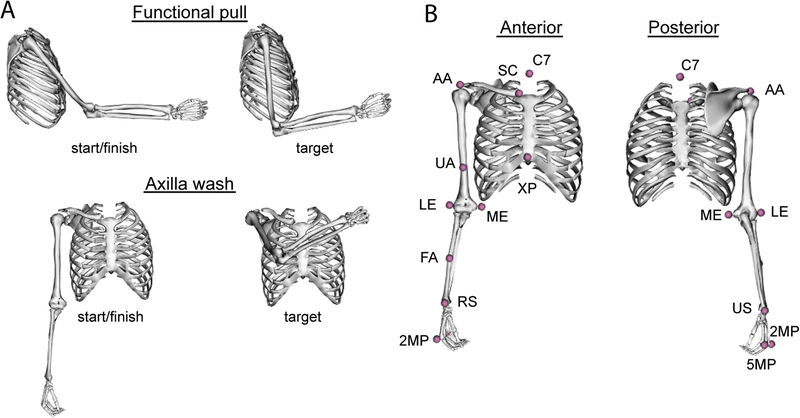
Background: Rotator cuff tears in older individuals may result in decreased muscle forces and changes to force distribution across the glenohumeral joint. Reduced muscle forces may impact functional task performance, altering glenohumeral joint contact forces, potentially contributing to instability or joint damage risk. Our objective was to evaluate the influence of rotator cuff muscle force distribution on glenohumeral joint contact force during functional pull and axilla wash tasks using individualized computational models.
Methods: Fourteen older individuals (age 63.4 yrs. (SD 1.8)) were studied; 7 with rotator cuff tear, 7 matched controls. Muscle volume measurements were used to scale a nominal upper limb model's muscle forces to develop individualized models and perform dynamic simulations of movement tracking participant-derived kinematics. Peak resultant glenohumeral joint contact force, and direction and magnitude of force components were compared between groups using ANCOVA.
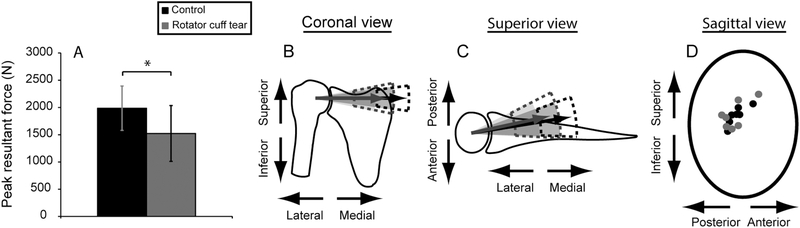
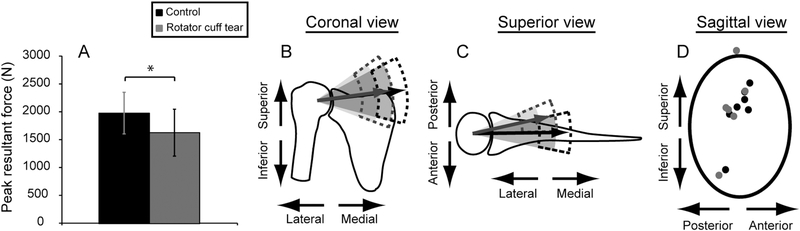
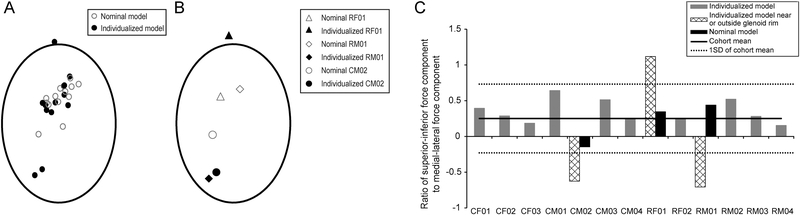
Findings: Results show individualized muscle force distributions for rotator cuff tear participants had reduced peak resultant joint contact force for pull and axilla wash (P ≤ 0.0456), with smaller compressive components of peak resultant force for pull (P = 0.0248). Peak forces for pull were within the glenoid. For axilla wash, peak joint contact was directed near/outside the glenoid rim for three participants; predictions required individualized muscle forces since nominal muscle forces did not affect joint force location.
Interpretation: Older adults with rotator cuff tear had smaller peak resultant and compressive forces, possibly indicating increased instability or secondary joint damage risk. Outcomes suggest predicted joint contact force following rotator cuff tear is sensitive to including individualized muscle forces.
Keywords: Computational model; Glenohumeral; Kinematics; Muscle forces; Older adult; Rotator cuff.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of Interest Statement
Author MTF declares that he serves as a consultant for Smith and Nephew. No financial compensation was received related to the information presented in this study and it does not represent a conflict of interest. Author CJT declares an ownership interest in a medical device that measures tension of rotator cuff tendon repairs and applications for research. Any development and testing of this device is unrelated to the study presented in this manuscript and does not represent a conflict of interest. No other authors have any conflicts of interest to disclose related to the work described in this manuscript.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
