

Outcome Prediction Using Perfusion Parameters and Collateral Scores of Multi-Phase and Single-Phase CT Angiography in Acute Stroke: Need for One, Two, Three, or Thirty Scans?
- PMID: 30309231
- PMCID: PMC6186923
- DOI: 10.5853/jos.2018.00605
Outcome Prediction Using Perfusion Parameters and Collateral Scores of Multi-Phase and Single-Phase CT Angiography in Acute Stroke: Need for One, Two, Three, or Thirty Scans?
Abstract
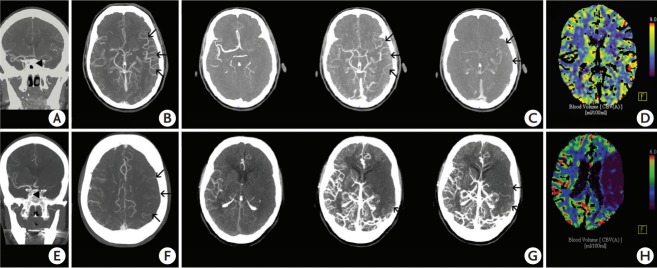
Background and purpose: Collateral status is an important factor determining outcome in acute ischemic stroke (AIS). Hence, different collateral scoring systems have been introduced. We applied different scoring systems on single- and multi-phase computed tomography (CT) angiography (spCTA and mpCTA) and compared them to CT perfusion (CTP) parameters to identify the best method for collateral evaluation in patients with AIS.
Methods: A total of 102 patients with AIS due to large vessel occlusion in the anterior circulation who underwent multimodal CT imaging and who were treated endovascularly were included. Collateral status was assessed on spCTA and mpCTA using four different scoring systems and compared to CTP parameters. Logistic regression was performed for predicting favorable outcome.
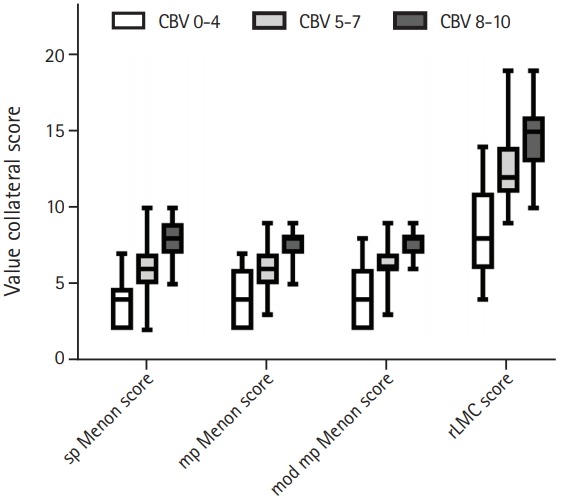
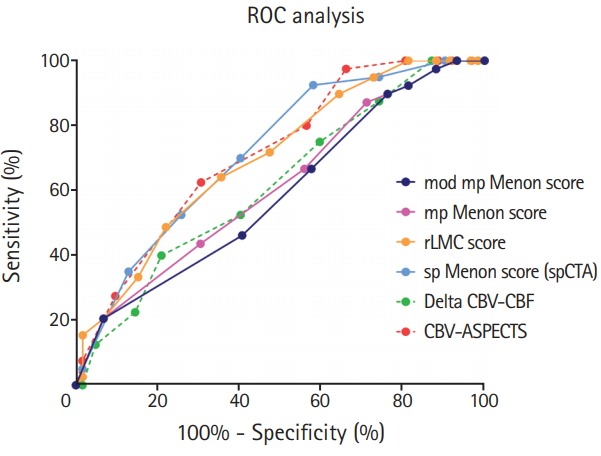
Results: All collateral scores correlated well with each other and with CTP parameters. Comparison of collateral scores stratified by extent of perfusion deficit showed relevant differences between groups (P<0.01 for each). An spCTA collateral score discriminated best between favorable and unfavorable outcome as determined using the modified Rankin Scale 3 months after stroke.
Conclusion: s Collateral status evaluated on spCTA may suffice for outcome prediction and decision making in AIS patients, potentially obviating further imaging modalities like mpCTA or CTP.
Keywords: Acute stroke; Collateral circulation; Computed tomography angiography; Perfusion; Treatment outcome.
Figures
References
-
- Sheth SA, Liebeskind DS. Collaterals in endovascular therapy for stroke. Curr Opin Neurol. 2015;28:10–15. - PubMed
-
- Elijovich L, Goyal N, Mainali S, Hoit D, Arthur AS, Whitehead M, et al. CTA collateral score predicts infarct volume and clinical outcome after endovascular therapy for acute ischemic stroke: a retrospective chart review. J Neurointerv Surg. 2016;8:559–562. - PubMed
-
- Gersing AS, Schwaiger BJ, Kleine JF, Kaesmacher J, Wunderlich S, Friedrich B, et al. Clinical outcome predicted by collaterals depends on technical success of mechanical thrombectomy in middle cerebral artery occlusion. J Stroke Cerebrovasc Dis. 2017;26:801–808. - PubMed
-
- Higashida R, Furlan A, Roberts H, Tomsick T, Connors B, Barr J, et al. Trial design and reporting standards for intraarterial cerebral thrombolysis for acute ischemic stroke. J Vasc Interv Radiol. 2003;14:S493–S494. - PubMed
-
- Ruland S, Ahmed A, Thomas K, Zhao M, Amin-Hanjani S, Du X, et al. Leptomeningeal collateral volume flow assessed by quantitative magnetic resonance angiography in large-vessel cerebrovascular disease. J Neuroimaging. 2009;19:27–30. - PubMed
LinkOut - more resources
Full Text Sources
