

Higher Blood Pressure during Endovascular Thrombectomy in Anterior Circulation Stroke Is Associated with Better Outcomes
- PMID: 30309232
- PMCID: PMC6186925
- DOI: 10.5853/jos.2018.01305
Higher Blood Pressure during Endovascular Thrombectomy in Anterior Circulation Stroke Is Associated with Better Outcomes
Abstract
Background and purpose: Reports investigating the relationship between in-procedure blood pressure (BP) and outcomes in patients undergoing endovascular thrombectomy (EVT) due to anterior circulation stroke are sparse and contradictory.
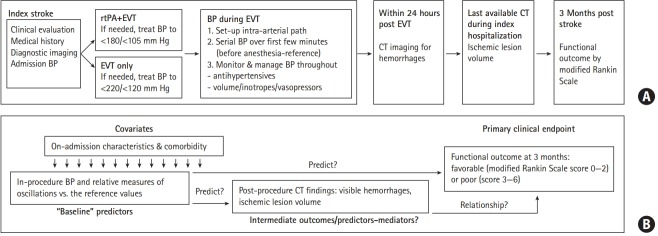
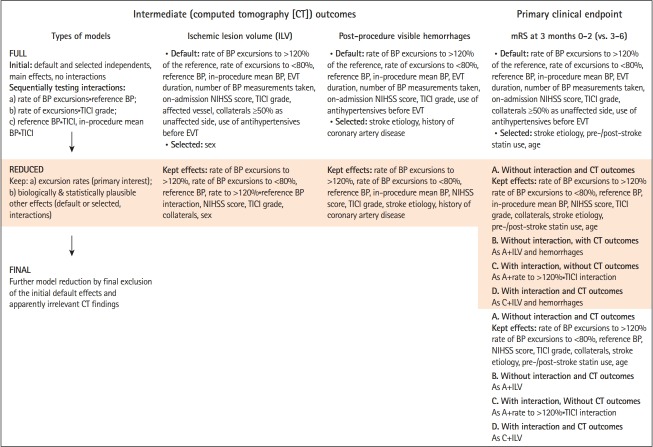
Methods: Consecutive EVT-treated adults (modern stent retrievers, BP managed in line with the recommendations, general anesthesia, invasive BP measurements) were evaluated for associations of the rate of in-procedure systolic BP (SBP) and mean arterial pressure (MAP) excursions to >120%/<80% of the reference values (serial measurements at anesthesia induction) and of the reference BP/weighted in-procedure mean BP with post-procedure imaging outcomes (ischemic lesion volume [ILV], hemorrhages) and 3-month functional outcome (modified Rankin Scale [mRS], score 0 to 2 vs. 3 to 6).
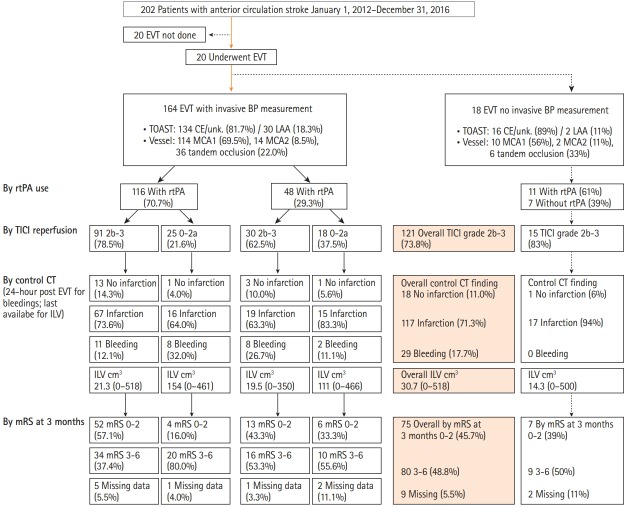
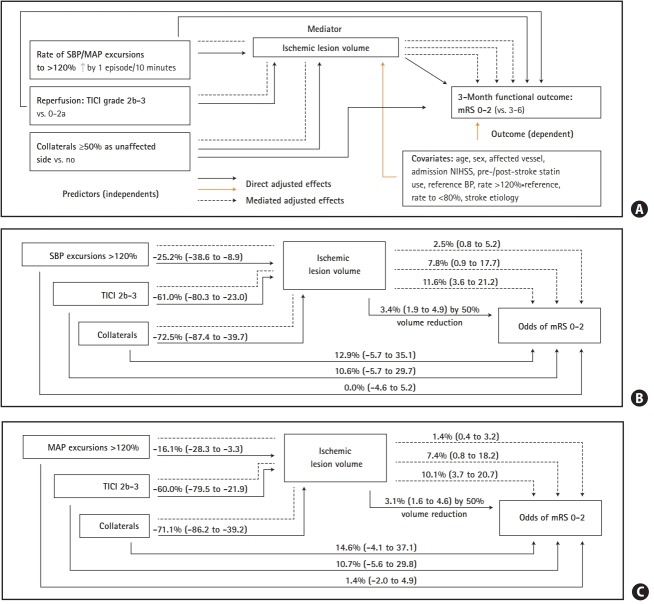
Results: Overall 164 patients (70.7% pharmacological reperfusion, 80.5% with good collaterals, 73.8% with successful reperfusion) were evaluated for ILV (range, 0 to 581 cm3) and hemorrhages (incidence 17.7%). Higher rate of in-procedure SBP/MAP excursions to >120% was independently associated with lower ILV, while higher in-procedure mean SBP/MAP was associated with lower odds of hemorrhages. mRS 0-2 was achieved in 75/155 (48.4%) evaluated patients (nine had missing mRS data). Higher rate of SBP/MAP excursions to >120% and higher reference SBP/MAP were independently associated with higher odds of mRS 0-2, while higher ILV was associated with lower odds of mRS 0-2. Rate of SBP/MAP excursions to <80% was not associated with any outcome.
Conclusion: s In the EVT-treated patients with BP managed within the recommended limits, a better functional outcome might be achieved by targeting in-procedure BP that exceeds the preprocedure values by more than 20%.
Keywords: Anesthesia, general; Blood pressure; Mechanical thrombolysis; Stroke.
Figures
References
-
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329. - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–e110. - PubMed
-
- Strandgaard S. Autoregulation of cerebral blood flow in hypertensive patients. The modifying influence of prolonged antihypertensive treatment on the tolerance to acute, druginduced hypotension. Circulation. 1976;53:720–727. - PubMed
LinkOut - more resources
Full Text Sources
