

Genomic Risk Prediction of Coronary Artery Disease in 480,000 Adults: Implications for Primary Prevention
- PMID: 30309464
- PMCID: PMC6176870
- DOI: 10.1016/j.jacc.2018.07.079
Genomic Risk Prediction of Coronary Artery Disease in 480,000 Adults: Implications for Primary Prevention
Abstract
Background: Coronary artery disease (CAD) has substantial heritability and a polygenic architecture. However, the potential of genomic risk scores to help predict CAD outcomes has not been evaluated comprehensively, because available studies have involved limited genomic scope and limited sample sizes.
Objectives: This study sought to construct a genomic risk score for CAD and to estimate its potential as a screening tool for primary prevention.
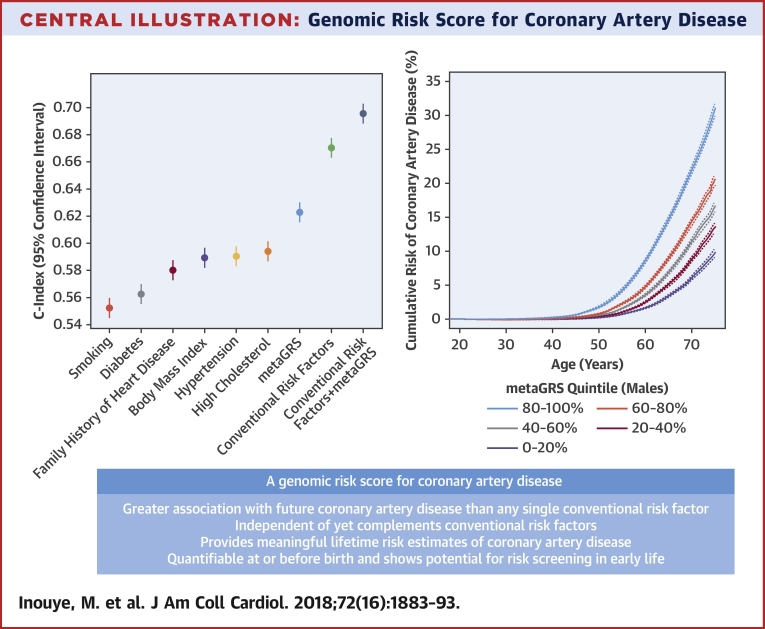
Methods: Using a meta-analytic approach to combine large-scale, genome-wide, and targeted genetic association data, we developed a new genomic risk score for CAD (metaGRS) consisting of 1.7 million genetic variants. We externally tested metaGRS, both by itself and in combination with available data on conventional risk factors, in 22,242 CAD cases and 460,387 noncases from the UK Biobank.
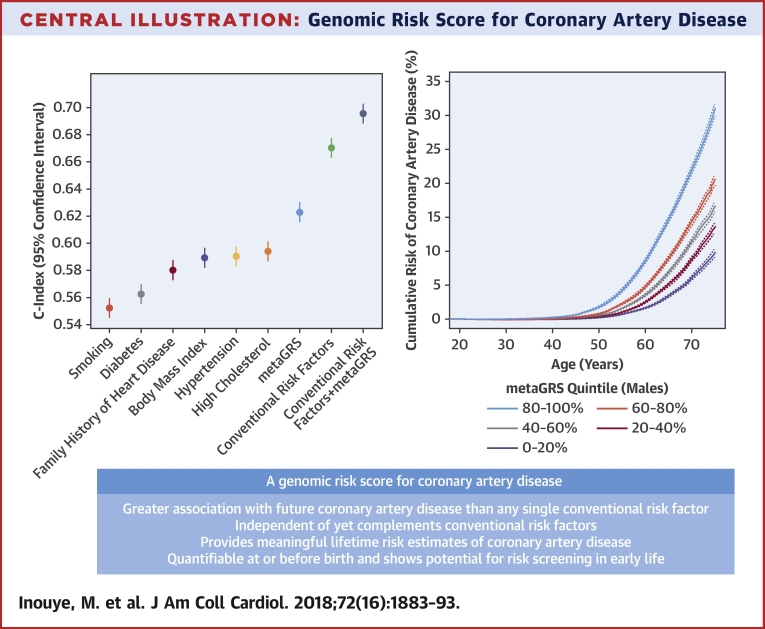
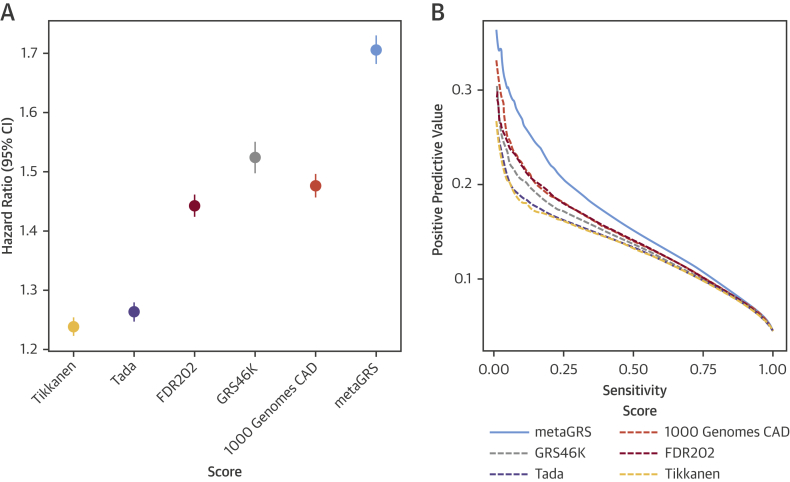
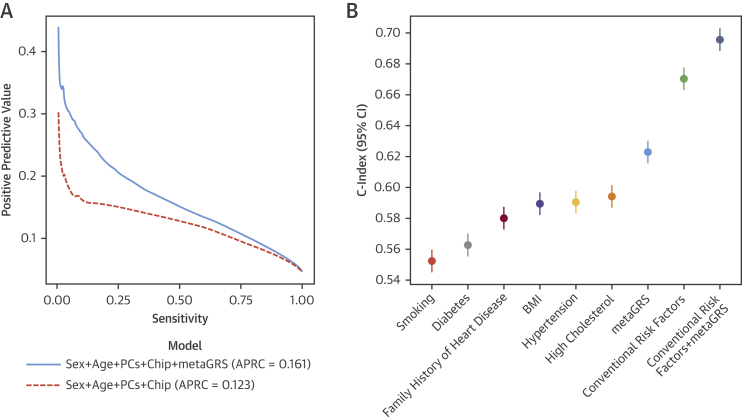
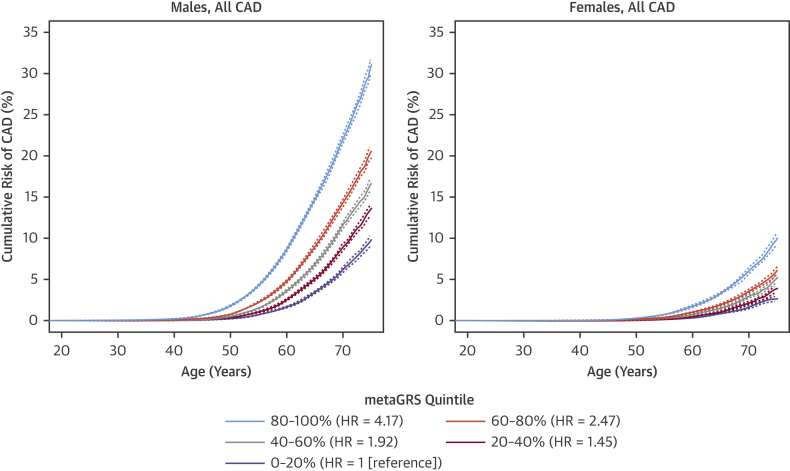
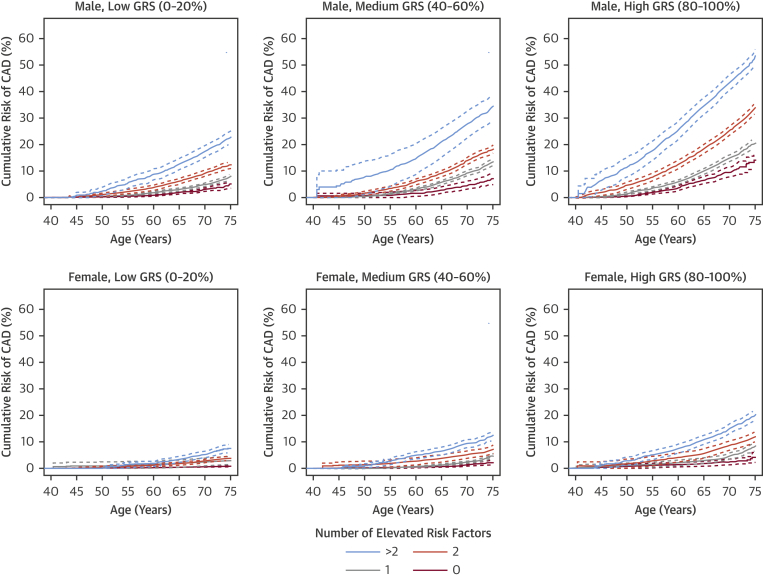
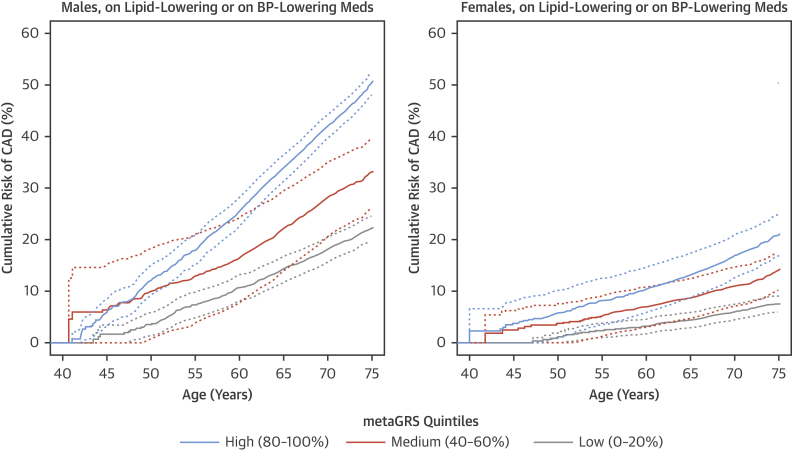
Results: The hazard ratio (HR) for CAD was 1.71 (95% confidence interval [CI]: 1.68 to 1.73) per SD increase in metaGRS, an association larger than any other externally tested genetic risk score previously published. The metaGRS stratified individuals into significantly different life course trajectories of CAD risk, with those in the top 20% of metaGRS distribution having an HR of 4.17 (95% CI: 3.97 to 4.38) compared with those in the bottom 20%. The corresponding HR was 2.83 (95% CI: 2.61 to 3.07) among individuals on lipid-lowering or antihypertensive medications. The metaGRS had a higher C-index (C = 0.623; 95% CI: 0.615 to 0.631) for incident CAD than any of 6 conventional factors (smoking, diabetes, hypertension, body mass index, self-reported high cholesterol, and family history). For men in the top 20% of metaGRS with >2 conventional factors, 10% cumulative risk of CAD was reached by 48 years of age.
Conclusions: The genomic score developed and evaluated here substantially advances the concept of using genomic information to stratify individuals with different trajectories of CAD risk and highlights the potential for genomic screening in early life to complement conventional risk prediction.
Keywords: coronary artery disease; genomic risk prediction; primary prevention.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Polygenic Risk Scoring for Coronary Heart Disease: The First Risk Factor.J Am Coll Cardiol. 2018 Oct 16;72(16):1894-1897. doi: 10.1016/j.jacc.2018.08.1041. J Am Coll Cardiol. 2018. PMID: 30309465 Free PMC article. No abstract available.
-
The illusion of polygenic disease risk prediction.Genet Med. 2019 Aug;21(8):1705-1707. doi: 10.1038/s41436-018-0418-5. Epub 2019 Jan 12. Genet Med. 2019. PMID: 30635622
References
-
- Watkins H., Farrall M. Genetic susceptibility to coronary artery disease: from promise to progress. Nat Rev Genet. 2006;7:163–173. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
