

Provider Specialty, Anticoagulation, and Stroke Risk in Patients With Atrial Fibrillation and Cancer
- PMID: 30309468
- PMCID: PMC6512871
- DOI: 10.1016/j.jacc.2018.07.077
Provider Specialty, Anticoagulation, and Stroke Risk in Patients With Atrial Fibrillation and Cancer
Abstract
Background: It is unknown whether early cardiology involvement shortly after atrial fibrillation (AF) diagnosis is associated with favorable outcomes in AF patients who have cancer.
Objectives: The purpose of this study was to examine the relationship between early cardiology involvement after AF diagnosis in patients with history of cancer.
Methods: This study examined associations of early cardiology involvement with oral anticoagulation use, stroke, and bleeding among nonvalvular AF patients (n = 388,045; mean age 68 ± 15 years; 59% male) with a history of cancer (past or active) from the MarketScan database (2009 to 2014). International Classification of Disease-9th Revision-Clinical Modification codes in any position were used to identify cancer diagnosis prior to AF diagnosis. Provider specialty and filled anticoagulant prescriptions 3 months prior to and 6 months after AF diagnosis were obtained. Poisson regression models were used to compute the probability of an oral anticoagulant prescription fill, and Cox regression was used to estimate the risks of stroke and major bleeding.
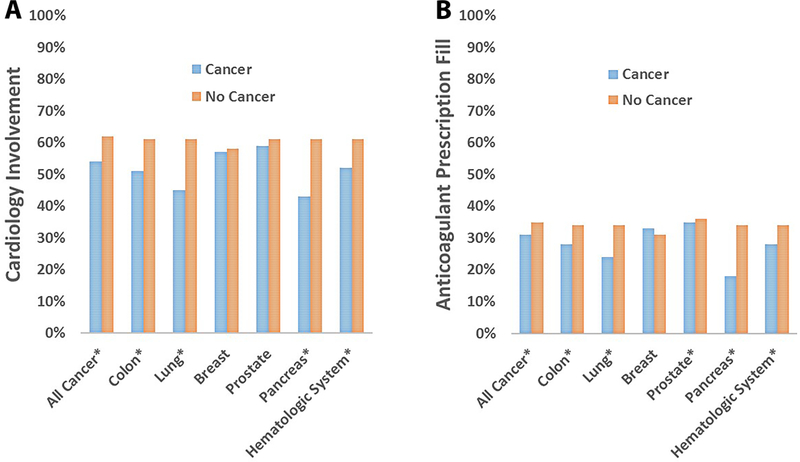
Results: A total of 64,016 (17%) AF patients had a history of cancer. Cardiology involvement was less likely to occur among patients with a history of cancer than those without (relative risk [RR]: 0.92 [95% confidence interval (CI): 0.91 to 0.93]). Patients with history of cancer were less likely to fill prescriptions for anticoagulants (RR: 0.89 [95% CI: 0.88 to 0.90]) than those without cancer, and similar results were observed across cancer types. Patients with cancer were more likely to fill prescriptions for anticoagulants (RR: 1.48 [95% CI: 1.45 to 1.52]) if seen by a cardiologist. A reduced risk of stroke (hazard ratio: 0.89 [95% CI: 0.81 to 0.99]) was observed among all cancer patients who were seen by a cardiology provider, without an increased risk of bleeding (hazard ratio: 1.04 [95% CI: 0.95 to 1.13]). Similar results were observed when the analysis was stratified by active versus remote history of cancer.
Conclusions: Although AF patients with cancer were less likely to see a cardiologist, or fill anticoagulant prescriptions, cardiology involvement was associated with increased anticoagulant prescription fills and favorable AF-related outcomes in AF patients with cancer.
Keywords: anticoagulation; atrial fibrillation; provider.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Atrial Fibrillation in Cancer Patients: Recognizing Gaps in Care.J Am Coll Cardiol. 2018 Oct 16;72(16):1923-1925. doi: 10.1016/j.jacc.2018.07.078. J Am Coll Cardiol. 2018. PMID: 30309469 No abstract available.
References
-
- Erichsen R, Christiansen CF, Mehnert F, Weiss NS, Baron JA, Sorensen HT. Colorectal cancer and risk of atrial fibrillation and flutter: a population-based case-control study. Intern Emerg Med 2012;7:431–8. - PubMed
-
- Guzzetti S, Costantino G, Vernocchi A, Sada S, Fundaro C. First diagnosis of colorectal or breast cancer and prevalence of atrial fibrillation. Intern Emerg Med 2008;3:227–31. - PubMed
-
- Melloni C, Shrader P, Carver J et al. Management and outcomes of patients with atrial fibrillation and a history of cancer: the ORBIT-AF registry. Eur Heart J Qual Care Clin Outcomes 2017;3:192–197. - PubMed
-
- Hu YF, Liu CJ, Chang PM et al. Incident thromboembolism and heart failure associated with new-onset atrial fibrillation in cancer patients. Int J Cardiol 2013;165:355–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
