

The need to improve access to rabies post-exposure vaccines: Lessons from Tanzania
- PMID: 30309746
- PMCID: PMC6863039
- DOI: 10.1016/j.vaccine.2018.08.086
The need to improve access to rabies post-exposure vaccines: Lessons from Tanzania
Abstract
Background: Rabies is preventable through prompt administration of post-exposure prophylaxis (PEP) to exposed persons, but PEP access is limited in many rabies-endemic countries. We investigated how access to PEP can be improved to better prevent human rabies.
Methods: Using data from different settings in Tanzania, including contact tracing (2,367 probable rabies exposures identified) and large-scale mobile phone-based surveillance (24,999 patient records), we estimated the incidence of rabies exposures and bite-injuries, and examined health seeking and health outcomes in relation to PEP access. We used surveys and qualitative interviews with stakeholders within the health system to further characterise PEP supply and triangulate these findings.
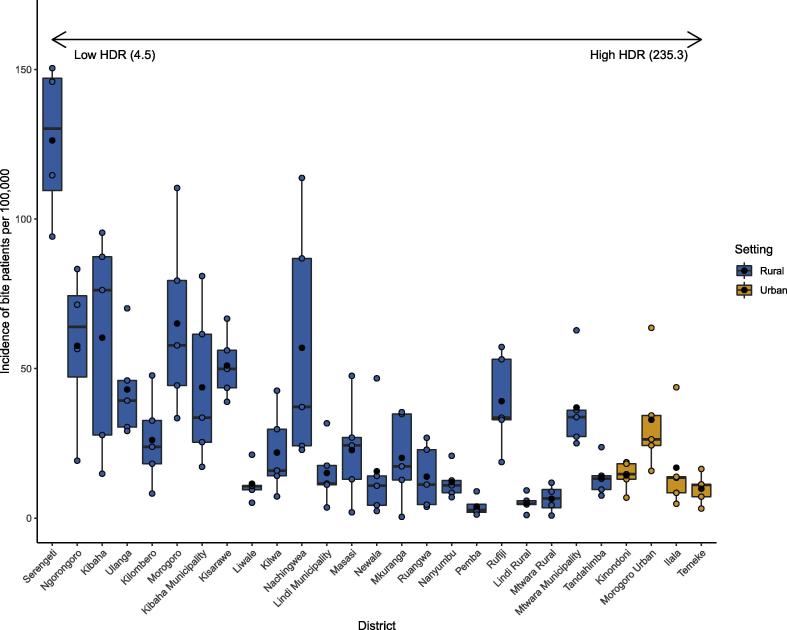
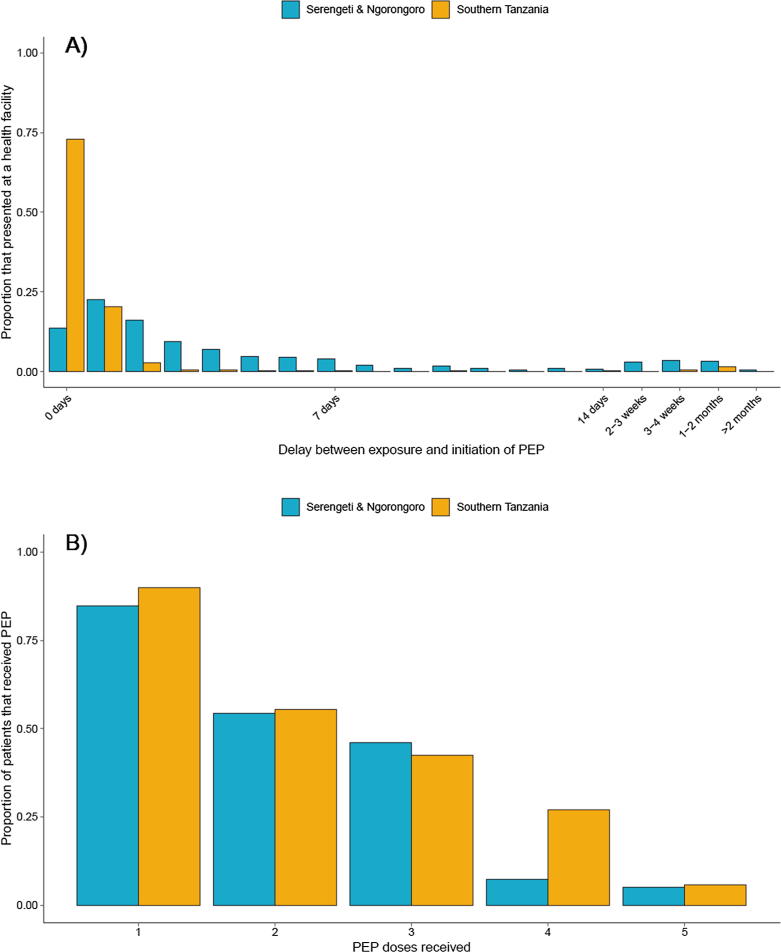
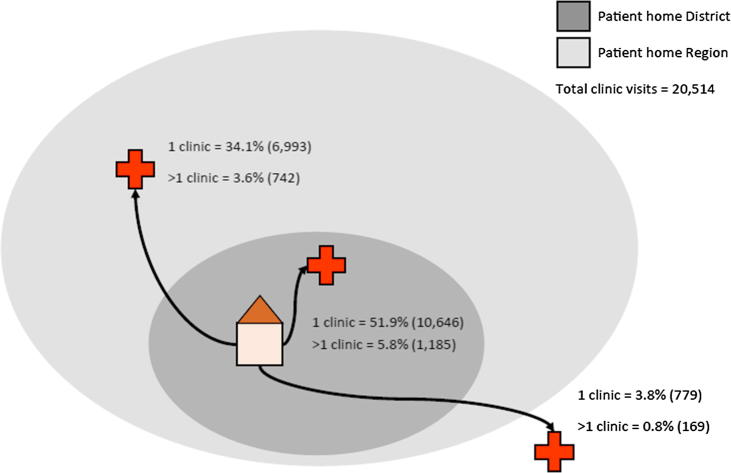
Results: Incidence of bite-injury patients was related to dog population sizes, with higher incidence in districts with lower human:dog ratios and urban centres. A substantial percentage (25%) of probable rabies exposures did not seek care due to costs and limited appreciation of risk. Upon seeking care a further 15% of probable rabies exposed persons did not obtain PEP due to shortages, cost barriers or misadvice. Of those that initiated PEP, 46% did not complete the course. If no PEP was administered, the risk of developing rabies following a probable rabies exposure was high (0.165), with bites to the head carrying most risk. Decentralized and free PEP increased the probability that patients received PEP and reduced delays in initiating PEP. No major difficulties were encountered by health workers whilst switching to dose-sparing ID administration of PEP. Health infrastructure also includes sufficient cold chain capacity to support improved PEP provision. However, high costs to governments and patients currently limits the supply chain and PEP access. The cost barrier was exacerbated by decentralization of budgets, with priority given to purchase of cheaper medicines for other conditions. Reactive procurement resulted in limited and unresponsive PEP supply, increasing costs and risks to bite victims.
Conclusion: PEP access could be improved and rabies deaths reduced through ring-fenced procurement, switching to dose-sparing ID regimens and free provision of PEP.
Keywords: Canine rabies; Dog-mediated rabies; Immunoglobulin; Intradermal; Intramuscular; Post-exposure prophylaxis; Procurement; Rabies prevention; Supply chain; Vaccine regimen.
Copyright © 2018. Published by Elsevier Ltd.
Figures
References
-
- World Health Organization. Rabies vaccine: WHO position paper – Weekly Epidemiological Record; 2018. Switzerland, 18, <http://www.who.int/rabies/resources/who_wer9316/en/>.
-
- Warrell M., Warrell D. Rabies and other lyssavirus diseases. The Lancet. 2004;363(9413):959–969. - PubMed
-
- Abela-Ridder B., Knopf L., Martin S., Taylor L., Torres G., De Balogh K. 2016: the beginning of the end of rabies? The Lancet Global Health. 2016;4(11):e780. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
