

Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review
- PMID: 30309799
- PMCID: PMC6185992
- DOI: 10.1016/S2214-109X(18)30398-X
Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review
Abstract
Background: Inadequate health-care provider performance is a major challenge to the delivery of high-quality health care in low-income and middle-income countries (LMICs). The Health Care Provider Performance Review (HCPPR) is a comprehensive systematic review of strategies to improve health-care provider performance in LMICs.
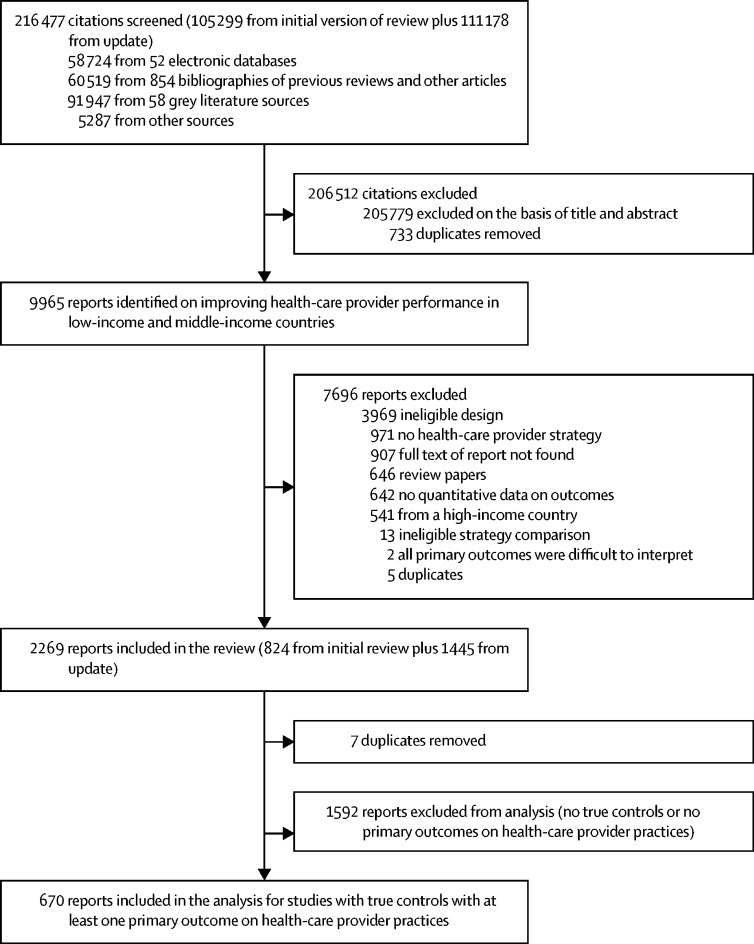
Methods: For this systematic review we searched 52 electronic databases for published studies and 58 document inventories for unpublished studies from the 1960s to 2016. Eligible study designs were controlled trials and interrupted time series. We only included strategy-versus-control group comparisons. We present results of improving health-care provider practice outcomes expressed as percentages (eg, percentage of patients treated correctly) or as continuous measures (eg, number of medicines prescribed per patient). Effect sizes were calculated as absolute percentage-point changes. The summary measure for each comparison was the median effect size (MES) for all primary outcomes. Strategy effectiveness was described with weighted medians of MES. This study is registered with PROSPERO, number CRD42016046154.
Findings: We screened 216 477 citations and selected 670 reports from 337 studies of 118 strategies. Most strategies had multiple intervention components. For professional health-care providers (generally, facility-based health workers), the effects were near zero for only implementing a technology-based strategy (median MES 1·0 percentage points, IQR -2·8 to 9·9) or only providing printed information for health-care providers (1·4 percentage points, -4·8 to 6·2). For percentage outcomes, training or supervision alone typically had moderate effects (10·3-15·9 percentage points), whereas combining training and supervision had somewhat larger effects than use of either strategy alone (18·0-18·8 percentage points). Group problem solving alone showed large improvements in percentage outcomes (28·0-37·5 percentage points), but, when the strategy definition was broadened to include group problem solving alone or other strategy components, moderate effects were more typical (12·1 percentage points). Several multifaceted strategies had large effects, but multifaceted strategies were not always more effective than simpler ones. For lay health-care providers (generally, community health workers), the effect of training alone was small (2·4 percentage points). Strategies with larger effect sizes included community support plus health-care provider training (8·2-125·0 percentage points). Contextual and methodological heterogeneity made comparisons difficult, and most strategies had low quality evidence.
Interpretation: The impact of strategies to improve health-care provider practices varied substantially, although some approaches were more consistently effective than others. The breadth of the HCPPR makes its results valuable to decision makers for informing the selection of strategies to improve health-care provider practices in LMICs. These results also emphasise the need for researchers to use better methods to study the effectiveness of interventions.
Funding: Bill & Melinda Gates Foundation, CDC Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Countdown to 2030 Collaboration Countdown to 2030: tracking progress towards universal coverage for reproductive, maternal, newborn, and child health. Lancet. 2018;391:1538–1548. - PubMed
-
- Hogerzeil HV, Liberman J, Wirtz VJ. Promotion of access to essential medicines for non-communicable diseases: practical implications of the UN political declaration. Lancet. 2013;381:680–689. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
