

CT and MR imaging of orbital inflammation
- PMID: 30310941
- PMCID: PMC6244997
- DOI: 10.1007/s00234-018-2103-4
CT and MR imaging of orbital inflammation
Abstract
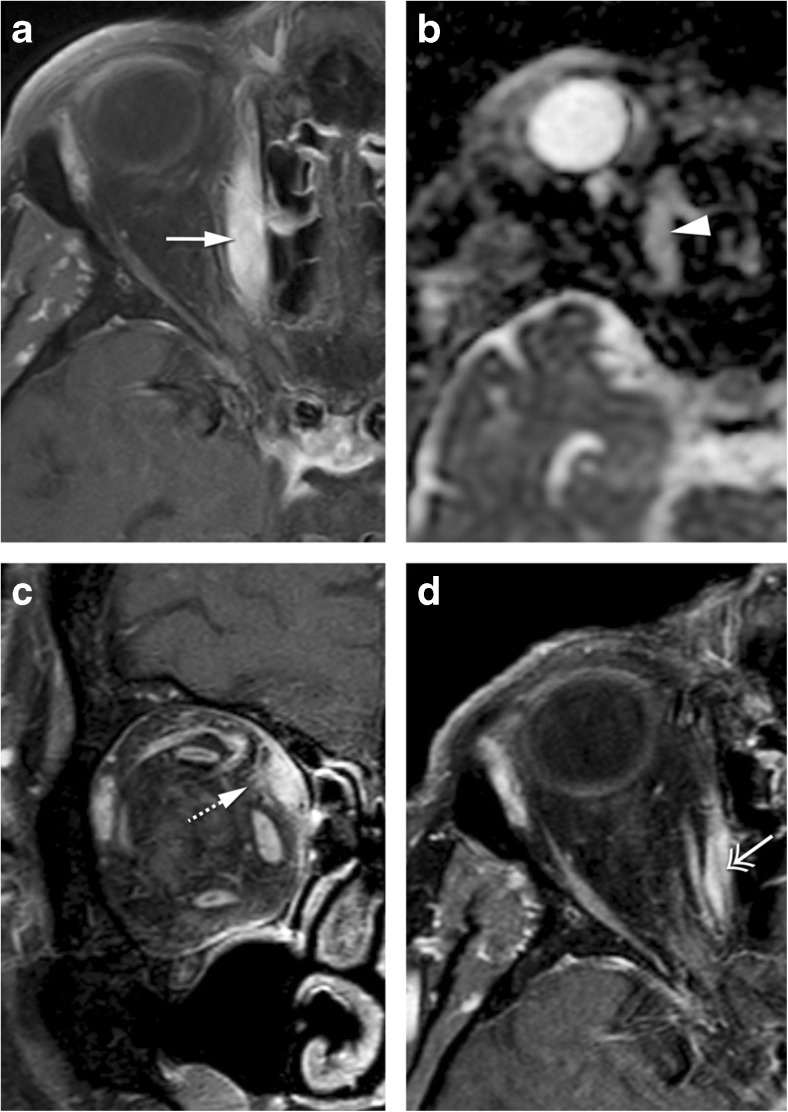
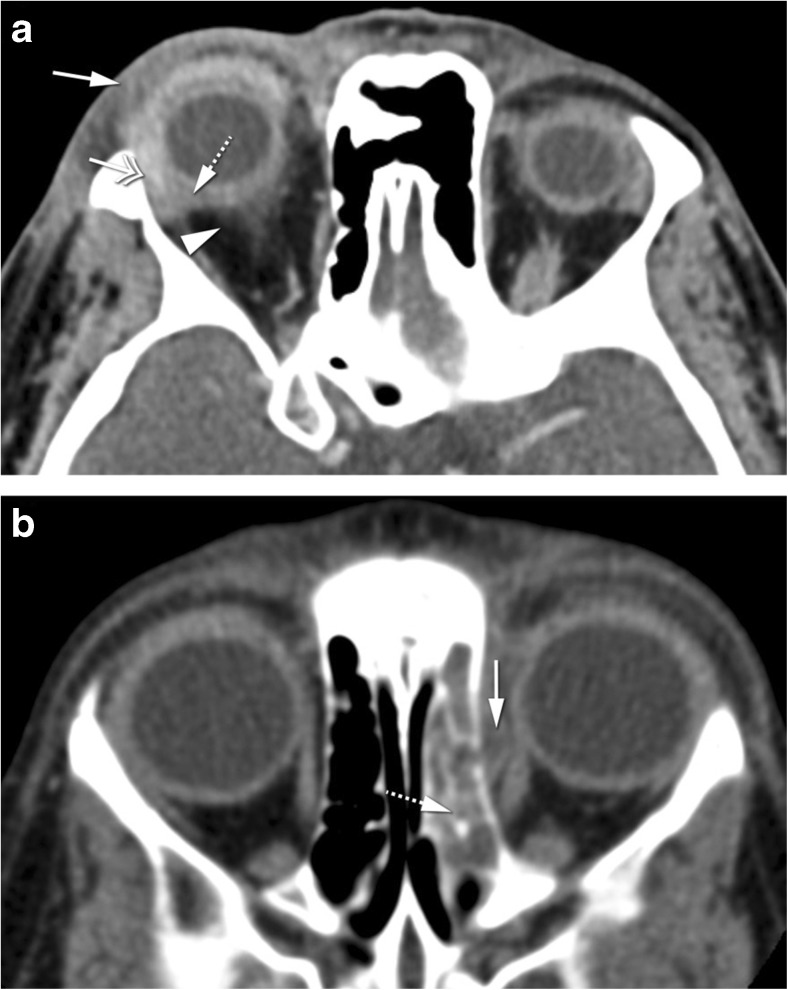
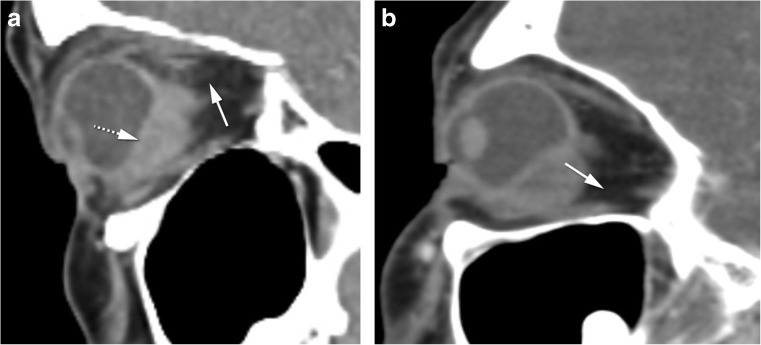
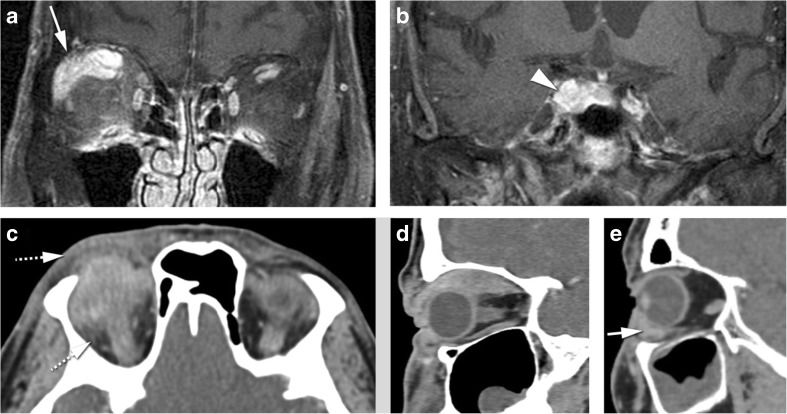
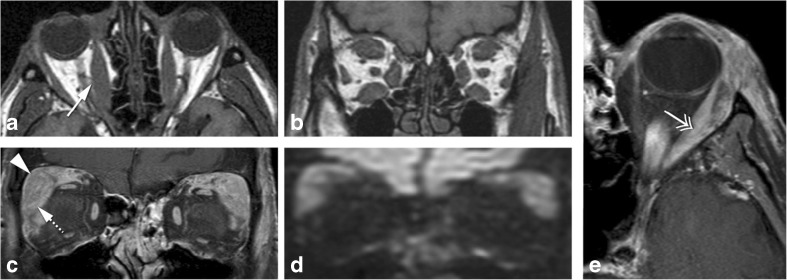
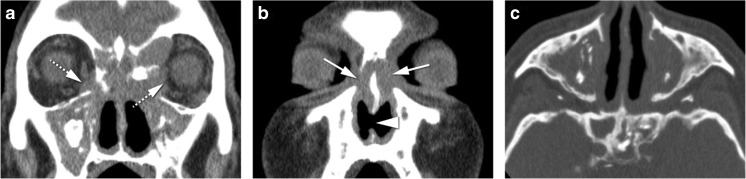
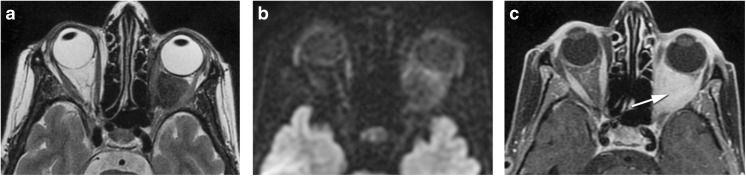
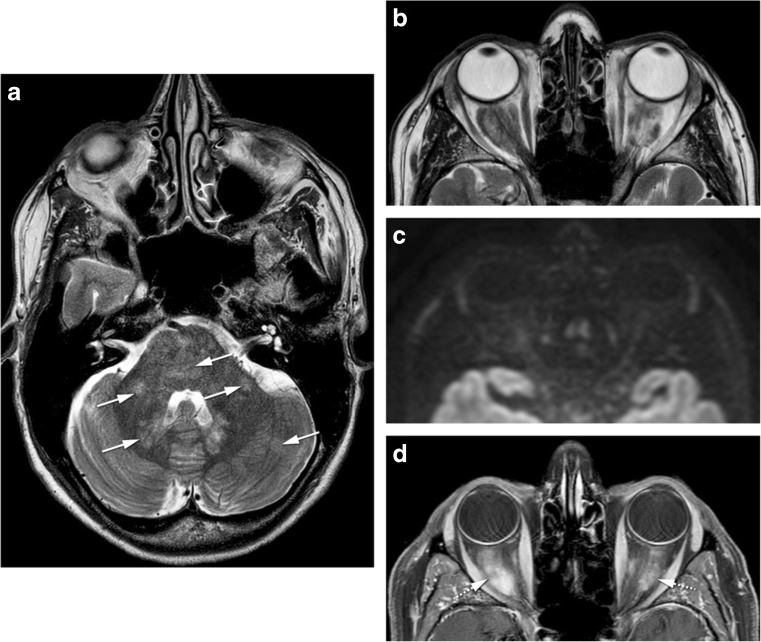
Purpose: Orbital inflammation can be idiopathic or in the context of a specific disease and it can involve different anatomical orbital structures. On imaging, inflammatory disease is frequently mistaken for infection and malignant tumors, and its underlying cause is often not determined. Through this article we aim to improve orbital inflammation diagnosis and underlying inflammatory diseases recognition.
Methods: The imaging protocols and characteristics of orbital inflammation were reviewed.
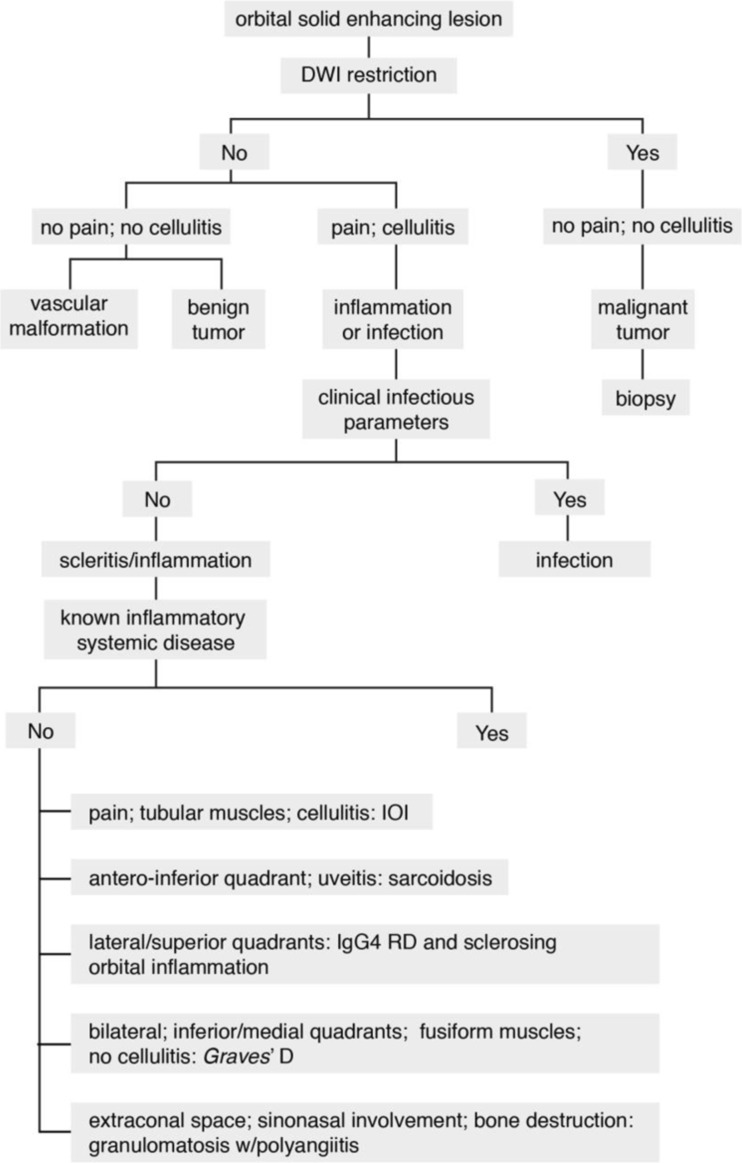
Results: A decision tree for the evaluation of these patients is provided. First, a combination of clinical and radiological clues is used to recognize inflammation, in particular to differentiate it both from orbital infection and tumor. Subsequently, different radiological patterns are recognized, often allowing the differentiation of the several orbital inflammatory diseases.
Conclusion: The use of adequate imaging protocols and subsequent evaluation allow the recognition of an orbital lesion as inflammatory and the diagnosis of the underlying inflammatory disease. All in all, a proper treatment can be established, and at times, a biopsy can be avoided.
Keywords: CT; Diffusion-weighted imaging; MRI; Orbital inflammation; Orbital inflammatory diseases.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study formal consent is not required.
Figures
References
-
- Wallace ZS, Khosroshahi A, Jakobiec FA, Deshpande V, Hatton MP, Ritter J, Ferry JA, Stone JH. IgG4-related systemic disease as a cause of “idiopathic” orbital inflammation, including orbital myositis, and trigeminal nerve involvement. Surv Ophthalmol. 2012;57:26–33. doi: 10.1016/j.survophthal.2011.07.004. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
