

Enteric duplication cysts in children: varied presentations, varied imaging findings
- PMID: 30311079
- PMCID: PMC6269332
- DOI: 10.1007/s13244-018-0660-z
Enteric duplication cysts in children: varied presentations, varied imaging findings
Abstract
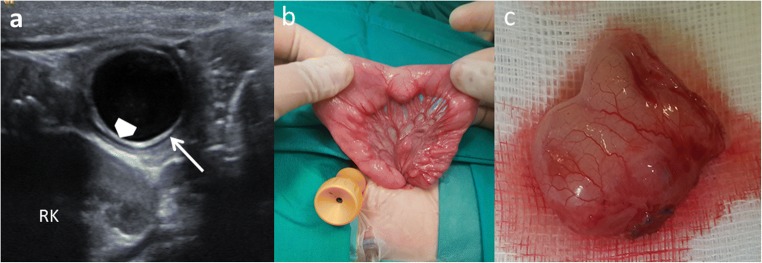
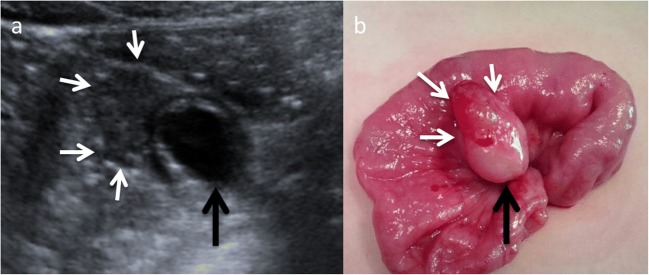
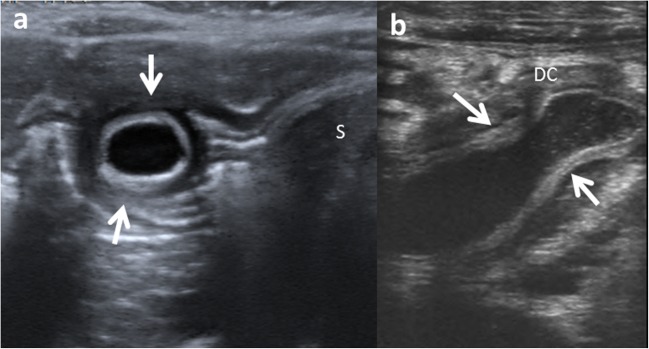
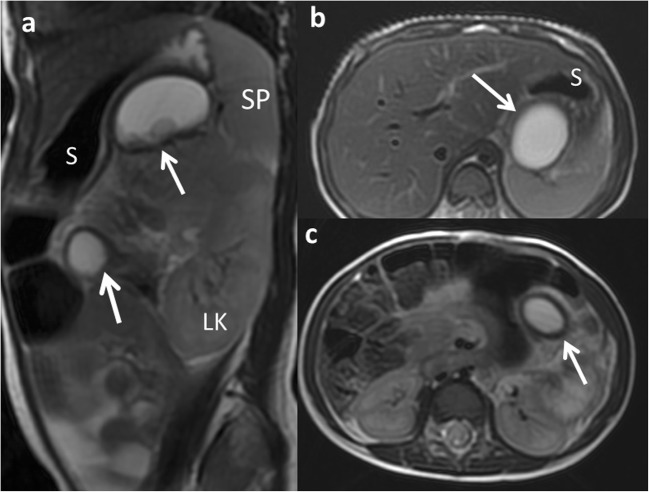
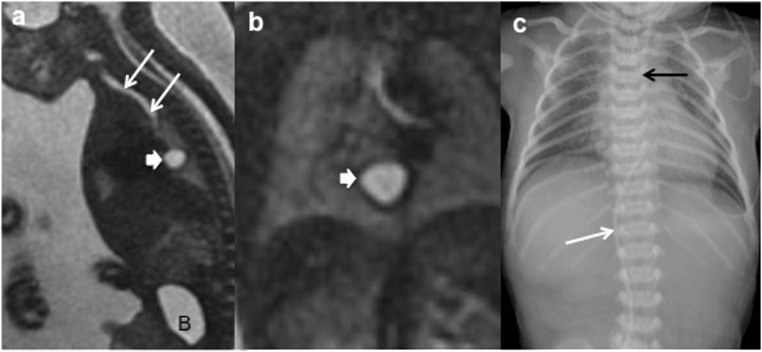
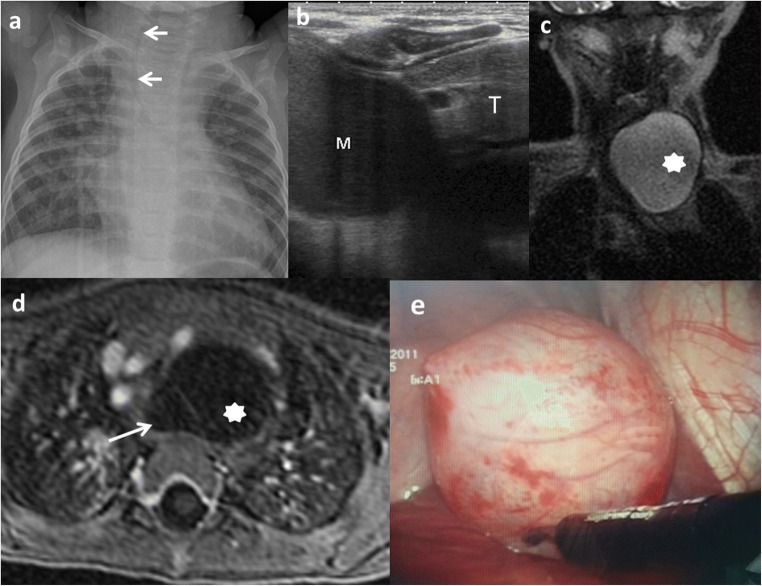
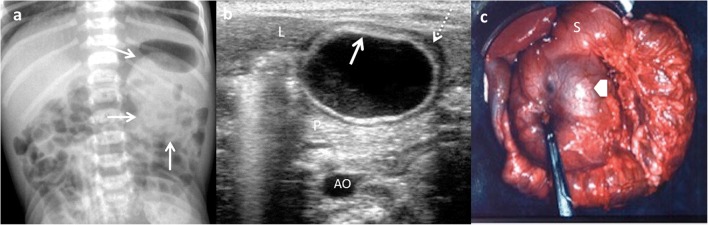
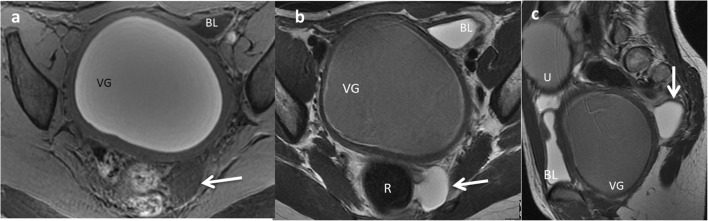
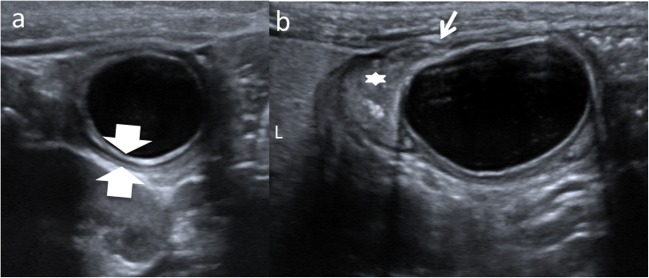
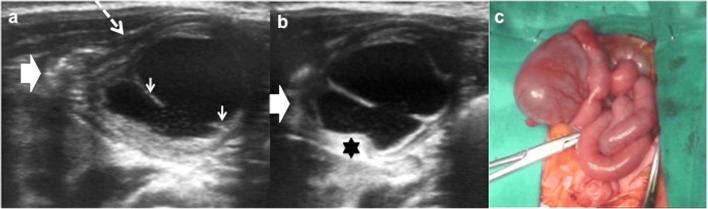
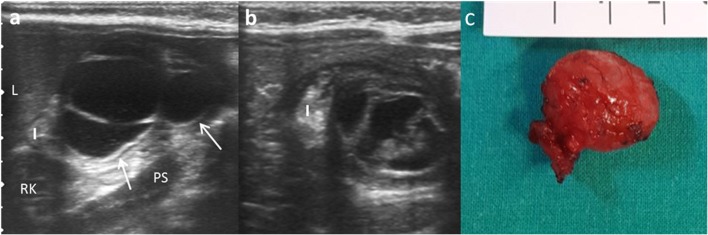
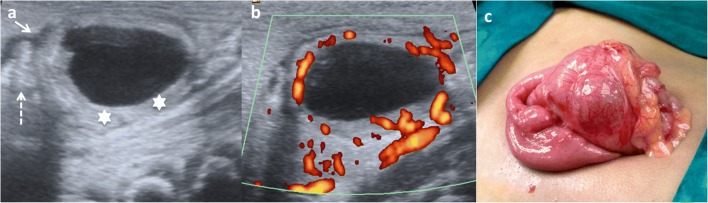
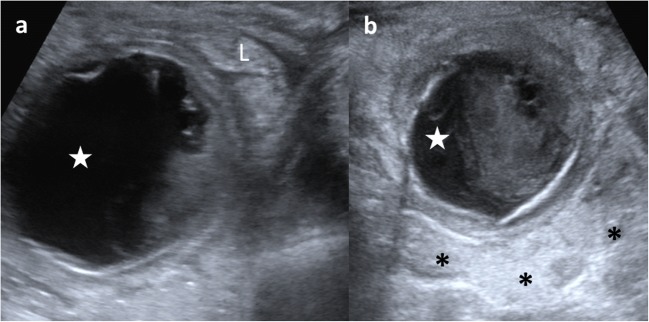
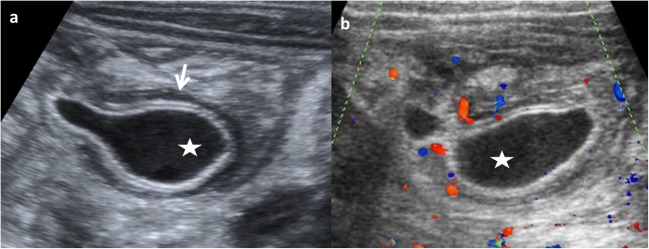
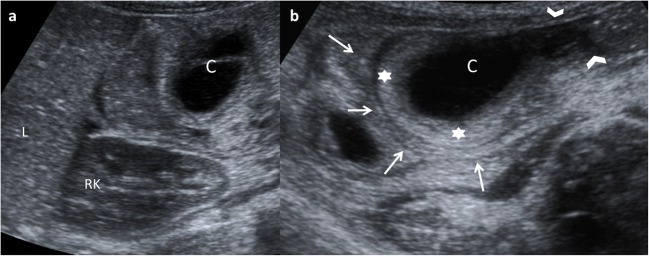
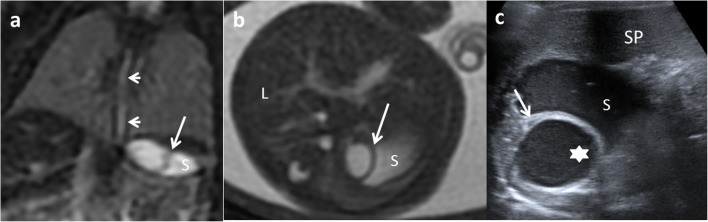
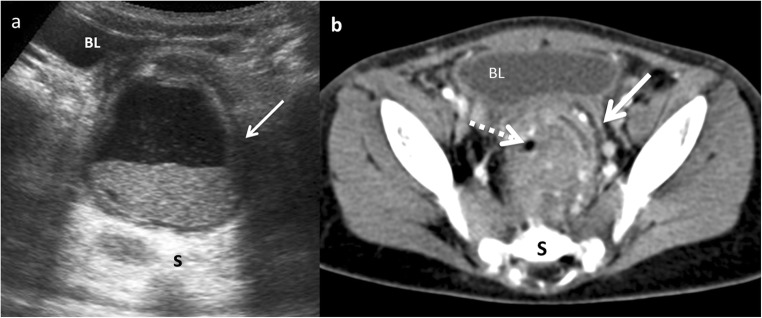
Enteric duplication cysts (EDCs) are rare congenital malformations formed during the embryonic development of the digestive tract. They are usually detected prenatally or in the first years of life. The size, location, type, mucosal pattern and presence of complications produce a varied clinical presentation and different imaging findings. Ultrasonography (US) is the most used imaging method for diagnosis. Magnetic resonance (MR) and computed tomography (CT) are less frequently used, but can be helpful in cases of difficult surgical approach. Conservative surgery is the treatment of choice. Pathology confirms the intestinal origin of the cyst, showing a layer of smooth muscle in the wall and an epithelial lining inside, resembling some part of the gastrointestinal tract (GT). We review the different forms of presentation of the EDCs, showing both the typical and atypical imaging findings with the different imaging techniques. We correlate the imaging findings with the surgical results and the final pathological features. TEACHING POINTS: • EDCs are rare congenital anomalies from the digestive tract with uncertain pathogenesis. • More frequently, diagnosis is antenatal, with most EDCs occurring in the distal ileum. • Ultrasonography is the method of choice for diagnosis of EDCs. • Complicated EDCs can show atypical imaging findings. • Surgery is necessary to avoid complications.
Keywords: Children; Cyst; Gastrointestinal tract; Magnetic resonance; Ultrasound.
Figures

References
-
- Berrocal T, Hidalgo P, Gutiérrez J, De Pablo L, Rodríguez-Lemos R. Imagen radiológica de las duplicaciones del tubo digestivo. Radiología. 2004;46:282–292. doi: 10.1016/S0033-8338(04)77978-3. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
