

Predictors of Survival for Patients with Acute Decompensated Heart Failure Requiring Extra-Corporeal Membrane Oxygenation Therapy
- PMID: 30312208
- PMCID: PMC6456436
- DOI: 10.1097/MAT.0000000000000898
Predictors of Survival for Patients with Acute Decompensated Heart Failure Requiring Extra-Corporeal Membrane Oxygenation Therapy
Abstract
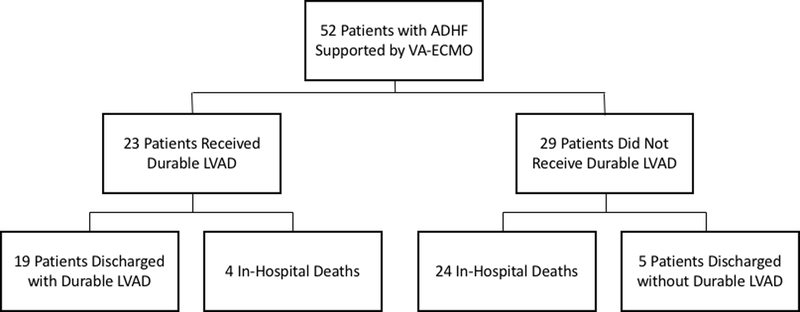
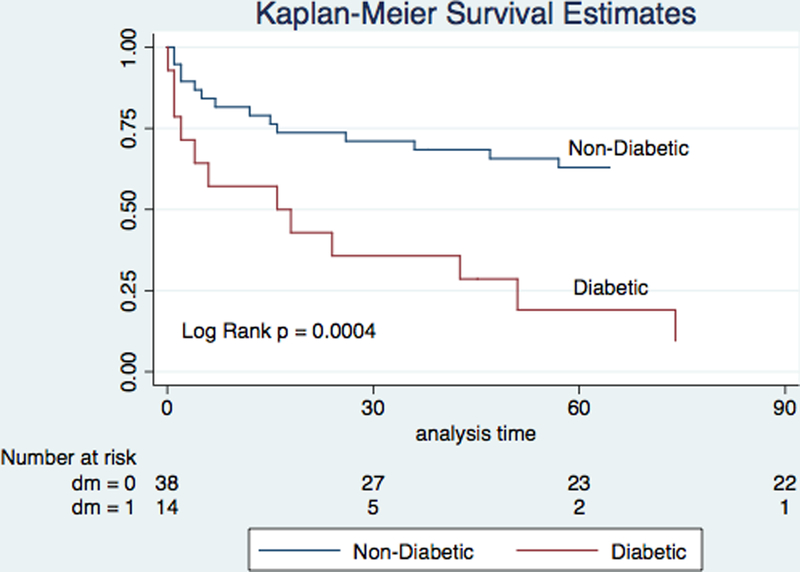
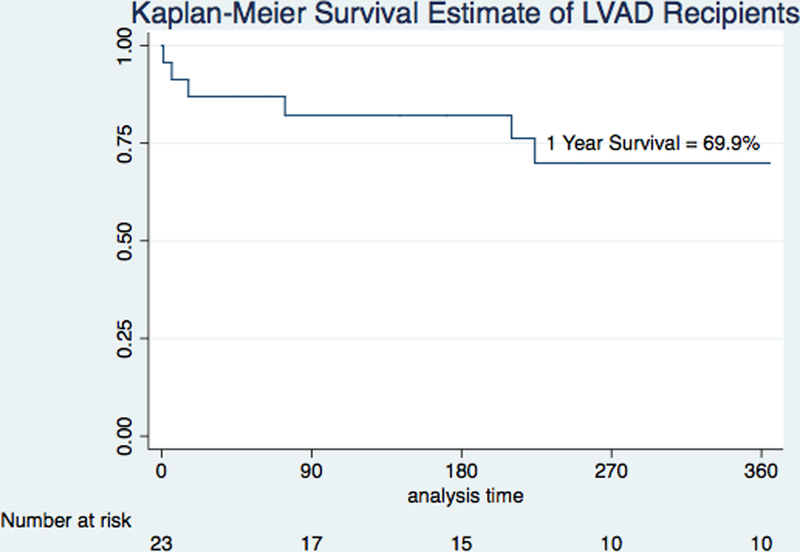
Chronic systolic heart failure (HF) with acute decompensation can result in cardiogenic shock (CS) requiring short-term mechanical circulatory support. We sought to identify predictors of survival for acute decompensated HF (ADHF) patients requiring veno-arterial extracorporeal membrane oxygenation (VA-ECMO). Patients >18 years old treated at our institution with VA-ECMO from 2009 to 2018 for ADHF with CS were studied. Demographic, hemodynamic, and echocardiographic data were collected. The primary outcome was survival to discharge. Fifty-two patients received VA-ECMO for ADHF with CS; 24 (46.2%) survived. Seventeen (32.7%) had suffered cardiac arrest, and 37 (71.2%) were mechanically ventilated. Mean lactate was 4.33 ± 3.45 mmol/L, and patients were receiving 2.7 ± 1.2 vasopressor/inotropic infusions at ECMO initiation; these did not differ significantly between survivors and nonsurvivors. Pre-ECMO cardiac index was 1.84 ± 0.56L/min/m and 1.94 ± 0.63L/min/m in survivors and nonsurvivors, respectively (p = 0.57). In multivariable analysis, only diabetes mellitus (DM; OR, 13.25; CI, 1.42-123.40; p = 0.02) and mineralocorticoid receptor antagonist use (OR, 0.12; CI, 0.02-0.78; p = 0.03) were independent predictors of mortality. Nineteen (79.2%) survivors required durable ventricular assist device. Among ADHF patients receiving VA-ECMO, DM is a powerful predictor of outcomes while markers of clinical acuity including hemodynamics, vasopressor/inotrope use, and lactate are not. The vast majority of survivors required durable left-ventricular assist devices.
Figures
References
-
- Goldberg RJ, Makam RC, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-Long Trends (2001–2011) in the Incidence and Hospital Death Rates Associated with the In-Hospital Development of Cardiogenic Shock after Acute Myocardial Infarction. Circ Cardiovasc Qual Outcomes. 2016;9:117–25. - PMC - PubMed
-
- Stretch R, Sauer CM, Yuh DD, Bonde P. National trends in the utilization of short-term mechanical circulatory support: incidence, outcomes, and cost analysis. J Am Coll Cardiol. 2014;64:1407–15. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart Failure (REMATCH) Study group. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med 2001;345:1435–1443. - PubMed
-
- Slaughter MS, Rogers JG, Milano CA, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med 2009;361:2241–2251. - PubMed
-
- Rogers JG, Aaronson KD, Boyle AJ, et al. Continuous flow left ventricular assist device improves functional capacity and quality of life of advanced heart failure patients. J Am Coll Cardiol. 2010;55:1826–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
