

Factors Associated With New Persistent Opioid Usage After Lung Resection
- PMID: 30316852
- PMCID: PMC7136012
- DOI: 10.1016/j.athoracsur.2018.08.057
Factors Associated With New Persistent Opioid Usage After Lung Resection
Abstract
Background: Opioid dependence, misuse, and abuse in the United States continue to rise. Prior studies indicate an important risk factor for persistent opioid use includes elective surgical procedures, though the probability following thoracic procedures remains unknown. We analyzed the incidence and factors associated with new persistent opioid use after lung resection.
Methods: We evaluated data from opioid-naïve cancer patients undergoing lung resection between 2010 and 2014 using insurance claims from the Truven Health MarketScan Databases. New persistent opioid usage was defined as continued opioid prescription fills between 90 and 180 days following surgery. Variables with a p value less than 0.10 by univariate analysis were included in a multivariable logistic regression performed for risk adjustment. Multivariable results were each reported with odds ratio (OR) and confidence interval (CI).
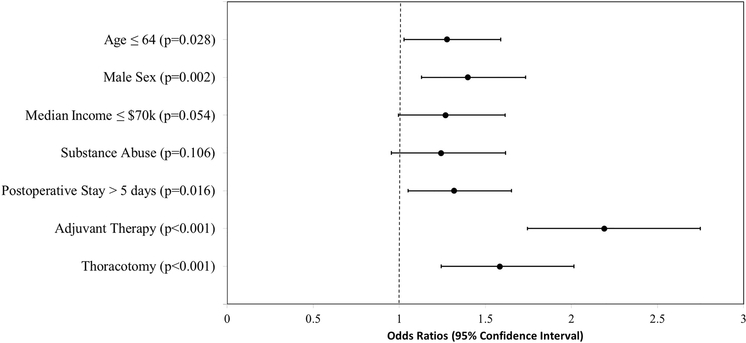
Results: A total of 3,026 patients (44.8% men, 55.2% women) were identified as opioid-naïve undergoing lung resection. Mean age was 64 ± 11 years and mean postoperative length of stay was 5.2 ± 3.3 days. A total of 6.5% underwent neoadjuvant therapy, while 21.7% underwent adjuvant therapy. Among opioid-naïve patients, 14% continued to fill opioid prescriptions following lung resection. Multivariable analysis showed that age less than or equal to 64 years (OR, 1.28; 95% CI, 1.03 to 1.59; p = 0.028), male sex (OR, 1.40; 95% CI, 1.13 to 1.73; p = 0.002), postoperative length of stay (OR, 1.32; 95% CI, 1.05 to 1.65; p = 0.016), thoracotomy (OR, 1.58; 95% CI, 1.24 to 2.02; p < 0.001), and adjuvant therapy (OR, 2.19; 95% CI, 1.75 to 2.75; p < 0.001) were independent risk factors for persistent opioid usage.
Conclusions: The greatest risk factors for persistent opioid use (14%) following lung resection were adjuvant therapy and thoracotomy. Future studies should focus on reducing excess prescribing, perioperative patient education, and safe opioid disposal.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Predictors of Opioid Prescription After Early Stage Lung Cancer Surgery.Ann Thorac Surg. 2019 Jun;107(6):1915. doi: 10.1016/j.athoracsur.2018.10.068. Epub 2018 Dec 6. Ann Thorac Surg. 2019. PMID: 30529668 No abstract available.
-
Reply.Ann Thorac Surg. 2019 Jun;107(6):1915-1916. doi: 10.1016/j.athoracsur.2018.12.050. Epub 2019 Jan 29. Ann Thorac Surg. 2019. PMID: 30707891 Free PMC article. No abstract available.
-
Predictors of Opioids on Discharge in Cardiothoracic Surgery in More Than 6000 Patients.Ann Thorac Surg. 2020 Jan;109(1):307. doi: 10.1016/j.athoracsur.2019.04.019. Epub 2019 May 15. Ann Thorac Surg. 2020. PMID: 31102637 No abstract available.
-
Reply.Ann Thorac Surg. 2020 Jan;109(1):307-308. doi: 10.1016/j.athoracsur.2019.06.036. Epub 2019 Aug 7. Ann Thorac Surg. 2020. PMID: 31400332 Free PMC article. No abstract available.
References
-
- Hedegaard H, Warner M, Minino AM. Drug overdose deaths in the United States, 1999–2016. NCHS data brief, no 294, Hyattsville, MD: National Center for Health Statistics, 2017. - PubMed
-
- Soneji N, Clarke HA, Ko DT, et al. Risks of Developing Persistent Opioid Use After Major Surgery. JAMA Surg 2016. November;151(11):1083–1084. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
