

Galunisertib plus gemcitabine vs. gemcitabine for first-line treatment of patients with unresectable pancreatic cancer
- PMID: 30318515
- PMCID: PMC6251034
- DOI: 10.1038/s41416-018-0246-z
Galunisertib plus gemcitabine vs. gemcitabine for first-line treatment of patients with unresectable pancreatic cancer
Abstract
Background: Galunisertib is the first-in-class, first-in-human, oral small-molecule type I transforming growth factor-beta receptor (ALK5) serine/threonine kinase inhibitor to enter clinical development. The effect of galunisertib vs. placebo in patients with unresectable pancreatic cancer was determined.
Methods: This was a two-part, multinational study: phase 1b was a non-randomised, open-label, multicentre, and dose-escalation study; phase 2 was a randomised, placebo- and Bayesian-augmented controlled, double-blind study in patients with locally advanced or metastatic pancreatic adenocarcinoma considered candidates for first-line chemotherapy with gemcitabine. Patients were randomised 2:1 to galunisertib-gemcitabine (N = 104) or placebo-gemcitabine (N = 52). Gemcitabine dose was 1000 mg/m2 QW. Primary endpoints for phases 1b and 2, respectively, were phase 2 dose and overall survival. Secondary objectives included tolerability and biomarkers.
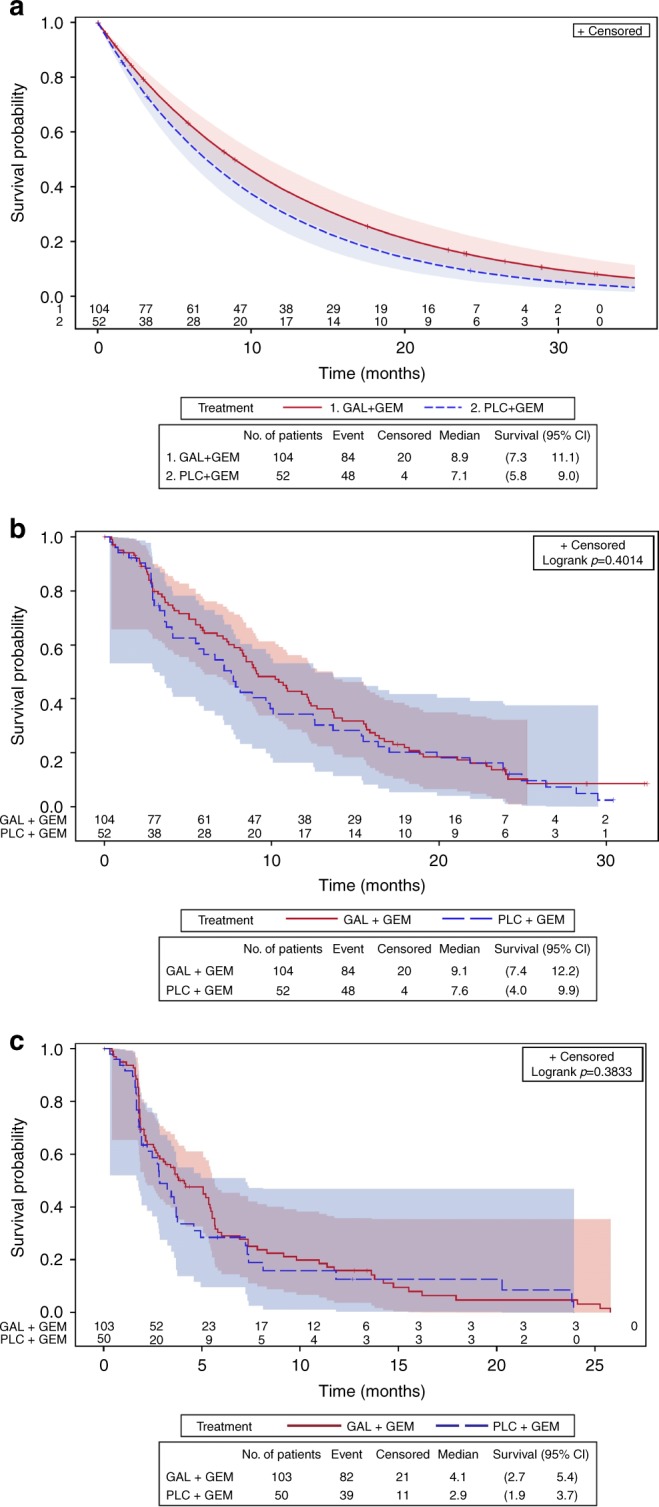
Results: Dose-escalation suggested a 300-mg/day dose. Primary objective was met: median survival times were 8.9 and 7.1 months for galunisertib and placebo, respectively (hazard ratio [HR] = 0.79 [95% credible interval: 0.59-1.09] and posterior probability HR < 1 = 0.93). Lower baseline biomarkers macrophage inflammatory protein-1-alpha and interferon-gamma-induced protein 10 were associated with galunisertib benefit.
Conclusions: Galunisertib-gemcitabine combination improved overall survival vs. gemcitabine in patients with unresectable pancreatic cancer, with minimal added toxicity. Future exploration of galunisertib in pancreatic cancer is ongoing in combination with durvalumab.
Conflict of interest statement
D.M. reports research funding from Shire, Incyte, and Celgene; a consulting role with Eli Lilly, Shire, Baxter and Incyte. G.D. reports research funding from Bavarian Nordici, Genentech, Janssen-Cilag, Roche, Sanofi, Eli Lilly, Exelixis, Sotio and Merck Serono; and travel fees from Roche, Amgen and Sanofi. M.F. reports a consulting role with Eli Lilly. J.T. reports a consulting role with Eli Lilly; speakers’ bureau from Bayer, Amgen and Merck Serono; and travel fees from Bayer. M.K. reports honorarium from Eli Lilly, Genentech, and Roche; a consulting role with Eli Lilly, Genentech, and Roche; and speakers’ bureau from Eli Lilly during the conduct of the study, Genentech, and Roche. A.C., C.S., S.T.E., I.G. and K.A.B. are all current employees and stockholders of Eli Lilly; M.M.F.L. is a former employee and stockholder of Eli Lilly and current employee of Incyte. A.B. is a current employee and stockholder of Advaxis, Inc. J.T. reports a consulting role with Eli Lilly, Amgen, Boehringer Ingelheim, Celgene, Chugai, Imclone, Merck, Merck Serono, Millenium, Novartis, Roche, Sanofi, Symphogen and Taiho. R.G.-C., T.M., D.P. and H.O. declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
