

Principles of TAVR valve design, modelling, and testing
- PMID: 30318937
- PMCID: PMC6417919
- DOI: 10.1080/17434440.2018.1536427
Principles of TAVR valve design, modelling, and testing
Abstract
Introduction: Transcatheter aortic valve replacement (TAVR) has emerged as an effective minimally-invasive alternative to surgical valve replacement in medium- to high-risk, elderly patients with calcific aortic valve disease and severe aortic stenosis. The rapid growth of the TAVR devices market has led to a high variety of designs, each aiming to address persistent complications associated with TAVR valves that may hamper the anticipated expansion of TAVR utility.
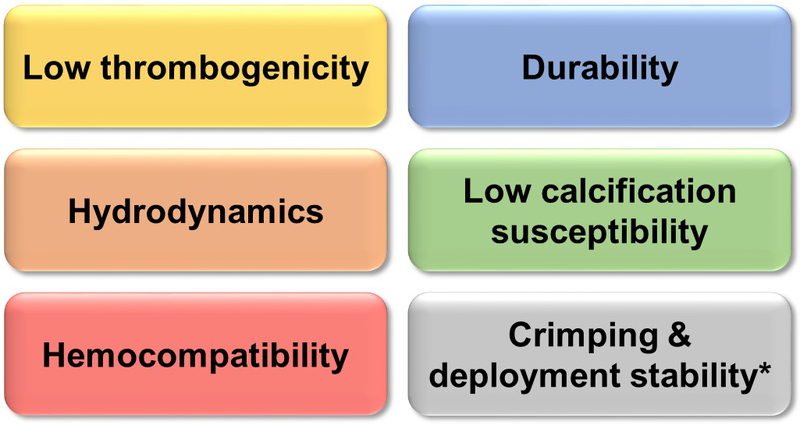
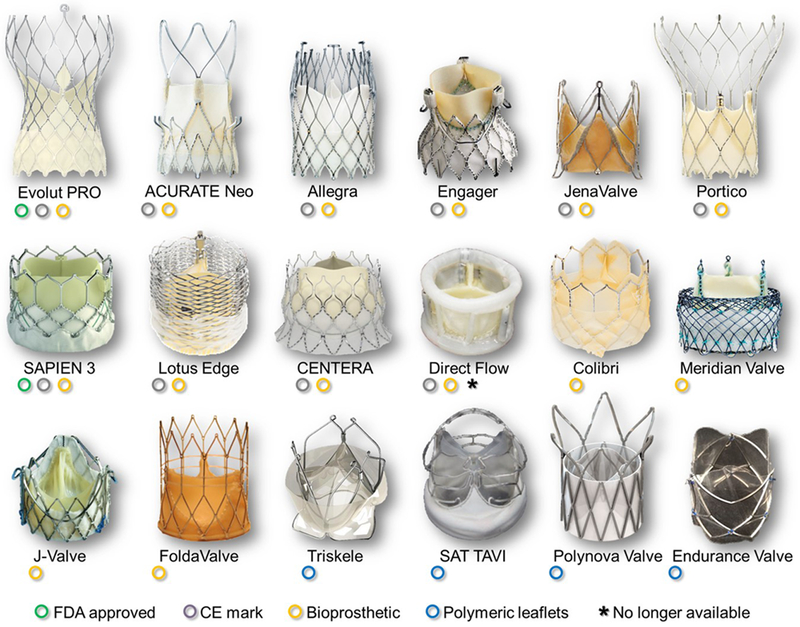
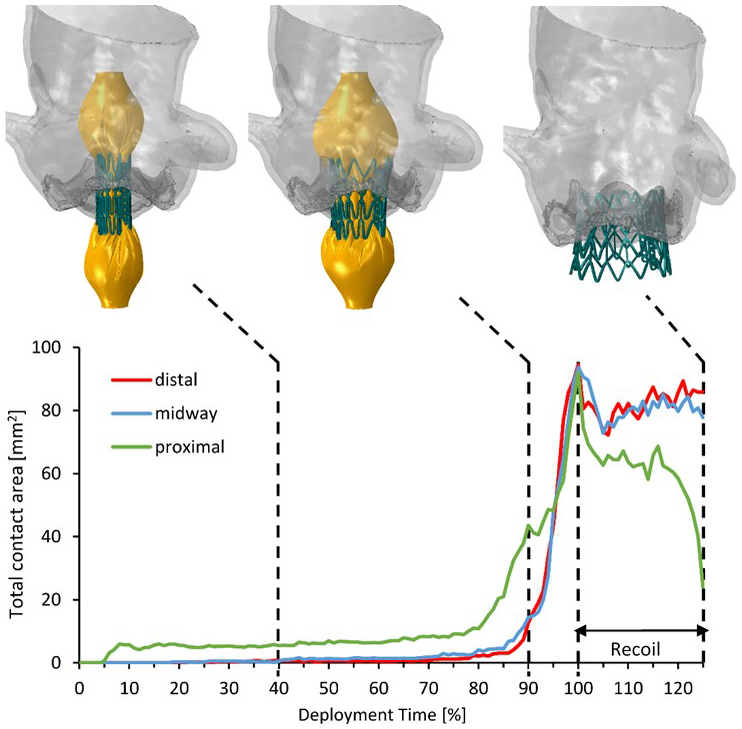
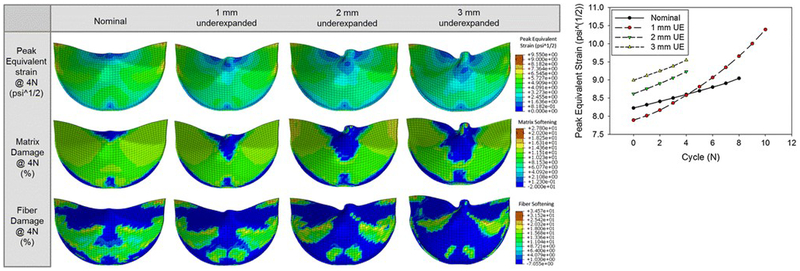
Areas covered: Here we outline the challenges and the technical demands that TAVR devices need to address for achieving the desired expansion, and review design aspects of selected, latest generation, TAVR valves of both clinically-used and investigational devices. We further review in detail some of the up-to-date modeling and testing approaches for TAVR, both computationally and experimentally, and additionally discuss those as complementary approaches to the ISO 5840-3 standard. A comprehensive survey of the prior and up-to-date literature was conducted to cover the most pertaining issues and challenges that TAVR technology faces.
Expert commentary: The expansion of TAVR over SAVR and to new indications seems more promising than ever. With new challenges to come, new TAV design approaches, and materials used, are expected to emerge, and novel testing/modeling methods to be developed.
Keywords: ISO 5840; TAVI; aortic stenosis; calcific aortic valve disease; medical device; prosthetic heart valve; thrombogenicity; valve hydrodynamics.
Conflict of interest statement
Declaration of interest
OM Rotman is a consultant for Polynova Cardiovascular Inc. D Bluestein has stock ownership in Polynova Cardiovascular Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
References
-
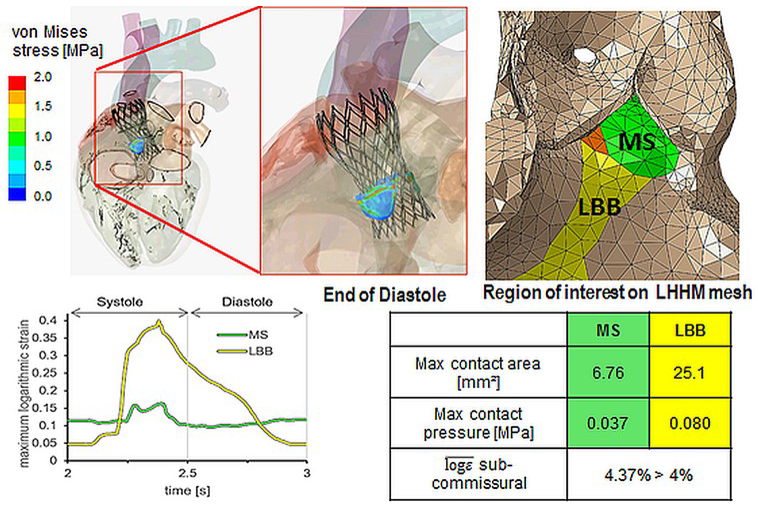
- Franzoni I, Latib A, Maisano F, et al. Comparison of incidence and predictors of left bundle branch block after transcatheter aortic valve implantation using the CoreValve versus the Edwards valve. The American journal of cardiology. 2013. August 15;112(4):554–9. doi: 10.1016/j.amjcard.2013.04.026. PubMed PMID: 23726173; eng. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources