

Mesalazine for People with Diverticular Disease: A Systematic Review of Randomized Controlled Trials
- PMID: 30320044
- PMCID: PMC6167594
- DOI: 10.1155/2018/5437135
Mesalazine for People with Diverticular Disease: A Systematic Review of Randomized Controlled Trials
Abstract
Background: Diverticular disease treatment is limited to fibres, antibiotics, and surgery. There is conflicting evidence on mesalazine benefits and harms.
Aim: We systematically reviewed current evidence on benefits and harms of mesalazine versus all other treatments in people with diverticular disease.
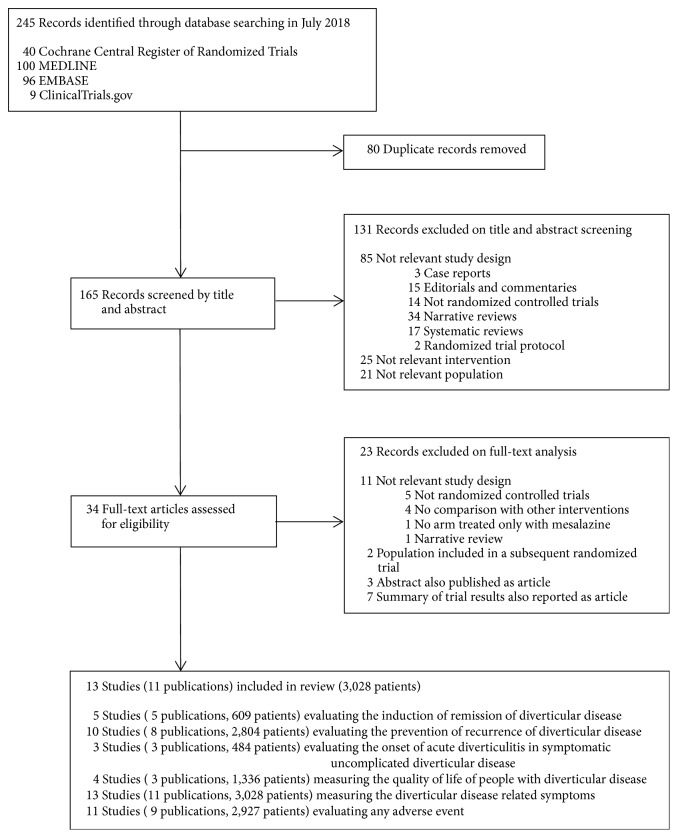
Methods: We searched MEDLINE, EMBASE, CENTRAL, ClinicalTrials.gov for studies published to July 2018. We estimated risk ratios (RR) for dichotomous outcomes (disease remission/recurrence, acute diverticulitis in symptomatic uncomplicated diverticular disease, need for surgery/hospitalization, all-cause/disease-related mortality, adverse events), mean differences (MD) or standardized MD (SMD) for continuous outcomes (quality of life, symptoms score, time to recurrence/remission), and their 95% confidence intervals (CI) using random-effects models. We quantified heterogeneity by Chi2 and I2 tests. We performed subgroup analyses by disease subtype, comparator, follow-up duration, mesalazine dose, and mode of administration.
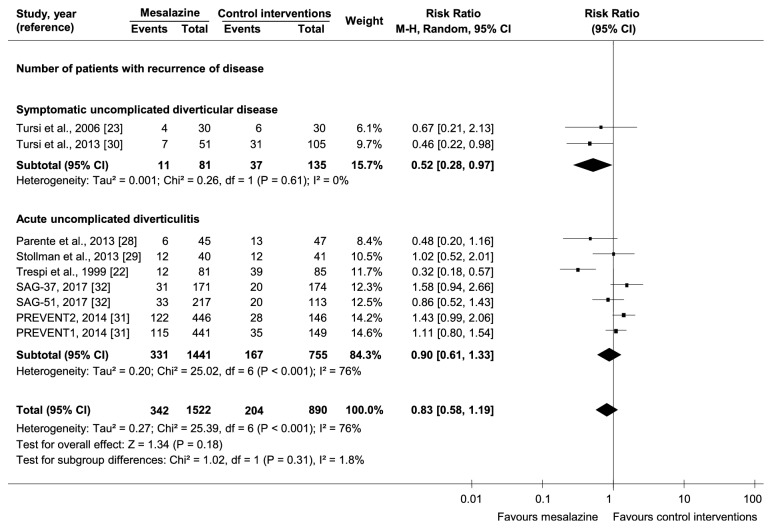
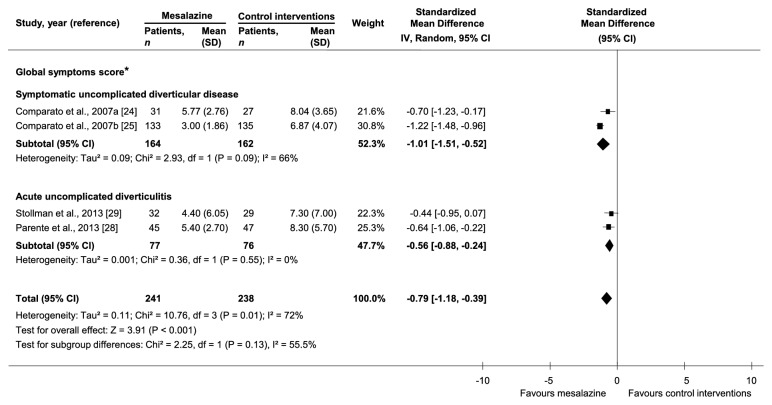
Results: We identified 13 randomized trials (n=3028 participants). There was a higher likelihood of disease remission with mesalazine than controls in acute uncomplicated diverticulitis (1 trial, 81 participants, RR=2.67, 95%CI=1.05-6.79), but not in symptomatic uncomplicated diverticular disease (1 trial, 123 participants, RR=1.04, 95%CI=0.81-1.34). There was a lower likelihood of disease recurrence with mesalazine than controls in symptomatic uncomplicated diverticular disease (2 trials, 216 participants, RR=0.52, 95%CI=0.28-0.97), but not in acute uncomplicated diverticulitis (7 trials, 2196 participants, RR=0.90, 95%CI=0.61-1.33). There was no difference in the likelihood of developing acute diverticulitis in symptomatic uncomplicated diverticular disease between the two groups (3 trials, 484 participants, RR=0.26, 95%CI=0.06-1.20). There was a higher global symptoms score reduction with mesalazine than controls in symptomatic uncomplicated diverticular disease (2 trials, 326 participants, SMD=-1.01, 95%CI=-1.51,-0.52) and acute uncomplicated diverticulitis (2 trials, 153 participants, SMD=-0.56, 95%CI=-0.88,-0.24).
Conclusions: Mesalazine may reduce recurrences in symptomatic uncomplicated diverticular disease. There is uncertainty on the effect of mesalazine in achieving diverticular disease remission. Mesalazine may not prevent acute diverticulitis in symptomatic uncomplicated diverticular disease.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
