

Family therapy approaches for anorexia nervosa
- PMID: 30320438
- PMCID: PMC6517149
- DOI: 10.1002/14651858.CD004780.pub3
Family therapy approaches for anorexia nervosa
Update in
-
Family therapy approaches for anorexia nervosa.Cochrane Database Syst Rev. 2019 May 1;5(5):CD004780. doi: 10.1002/14651858.CD004780.pub4. Cochrane Database Syst Rev. 2019. PMID: 31041816 Free PMC article.
Abstract
Background: Anorexia nervosa (AN) is characterised by a failure to maintain a normal body weight due to a paucity of nutrition, an intense fear of gaining weight or behaviour that prevents the individual from gaining weight, or both. The long-term prognosis is often poor, with severe developmental, medical and psychosocial complications, high rates of relapse and mortality. 'Family therapy approaches' indicate a range of approaches, derived from different theories, that involve the family in treatment. We have included therapies developed on the basis of dominant family systems theories, approaches that are based on or broadly similar to the family-based therapy derived from the Maudsley model, approaches that incorporate a focus on cognitive restructuring, as well as approaches that involve the family without articulation of a theoretical approach.This is an update of a Cochrane Review first published in 2010.
Objectives: To evaluate the efficacy of family therapy approaches compared with standard treatment and other treatments for AN.
Search methods: We searched the Cochrane Common Mental Disorders Controlled Trials Register (CCMDCTR) and PsycINFO (OVID) (all years to April 2016). We ran additional searches directly on Cochrane Central Register for Controlled Trials (CENTRAL), MEDLINE, Ovid Embase, and PsycINFO (to 2008 and 2016 to 2018). We searched the World Health Organization (WHO) trials portal (ICTRP) and ClinicalTrials.gov, together with four theses databases (all years to 2018). We checked the reference lists of all included studies and relevant systematic reviews. We have included in the analyses only studies from searches conducted to April 2016.
Selection criteria: Randomised controlled trials (RCTs) of family therapy approaches compared to any other intervention or other types of family therapy approaches were eligible for inclusion. We included participants of any age or gender with a primary clinical diagnosis of anorexia nervosa.
Data collection and analysis: Four review authors selected the studies, assessed quality and extracted data. We used a random-effects meta-analysis. We used the risk ratio (with a 95% confidence interval) to summarise dichotomous outcomes and both the standardised mean difference and the mean difference to summarise continuous measures.
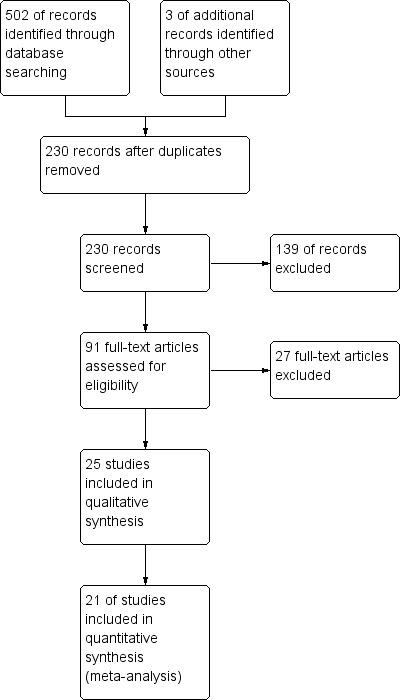
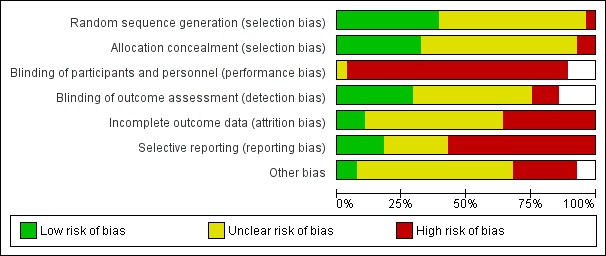
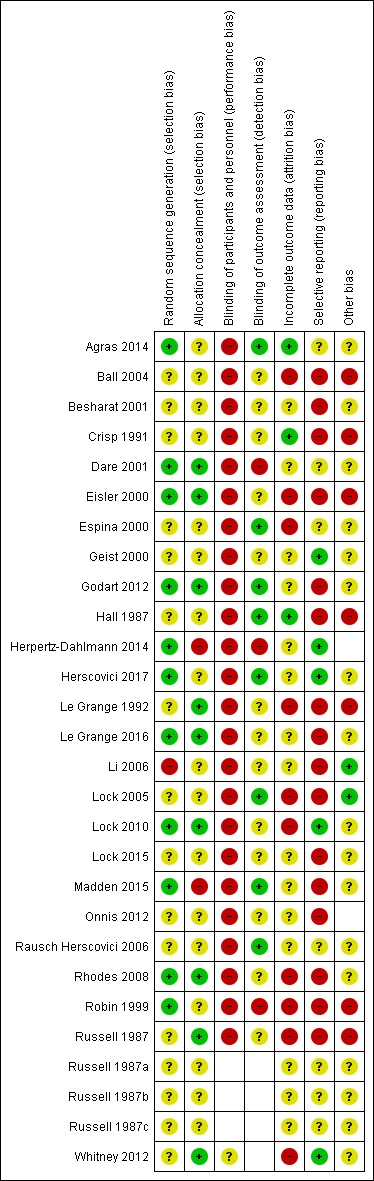
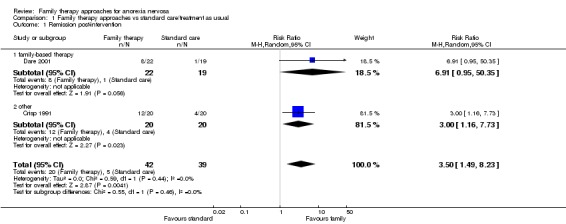
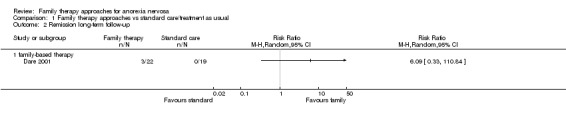
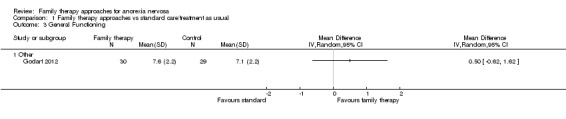
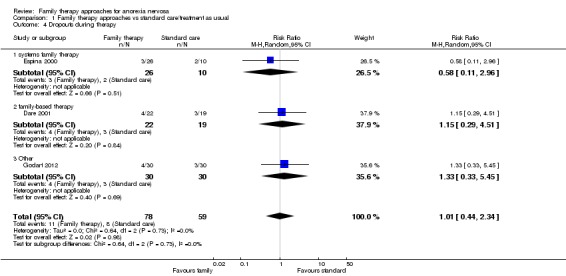
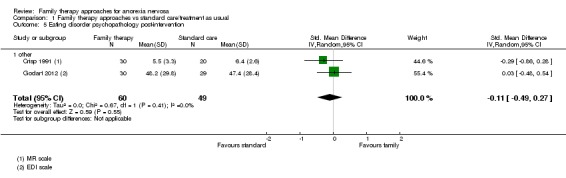
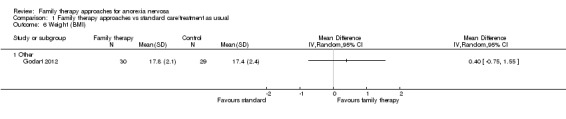
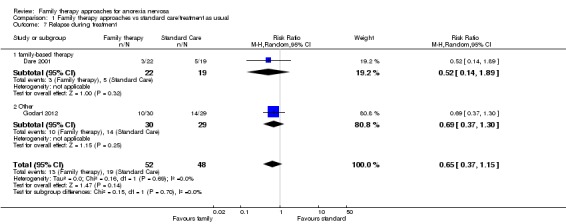
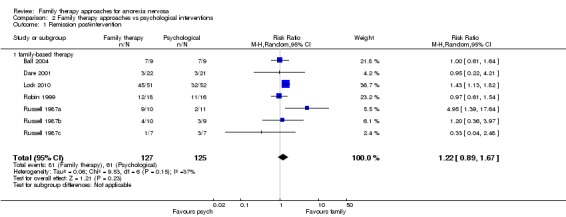
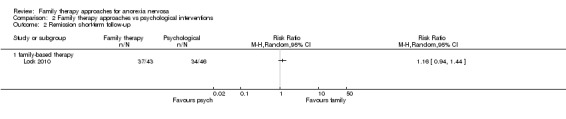
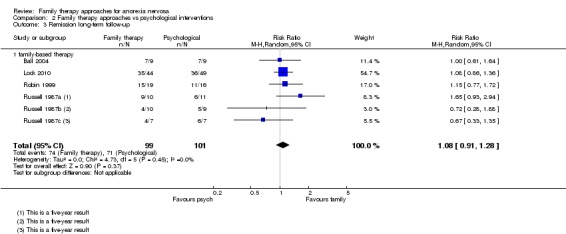
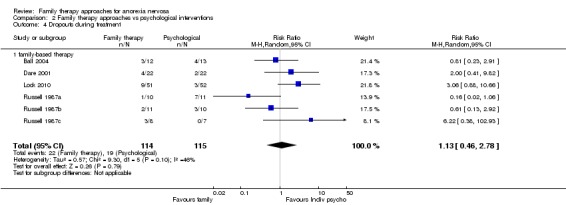
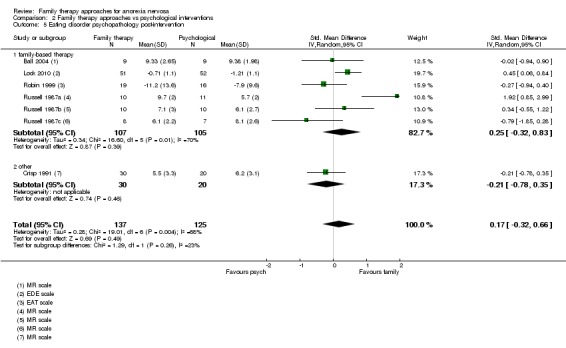
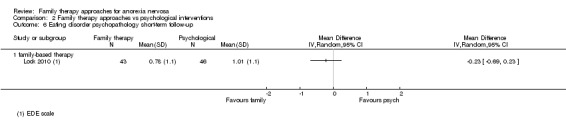
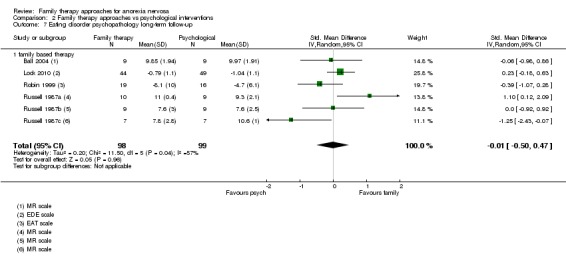
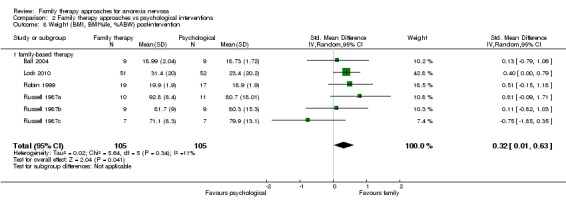
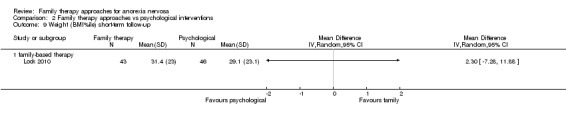
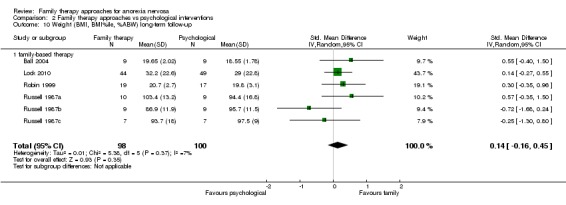
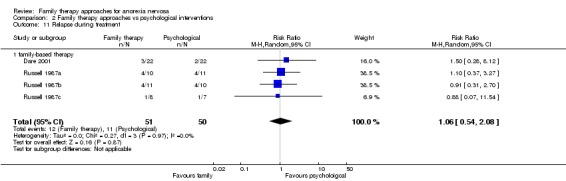
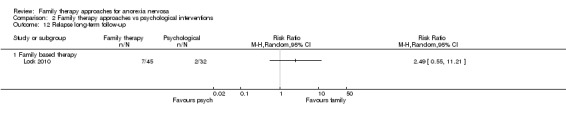
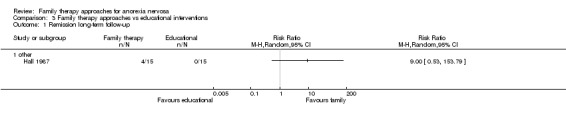
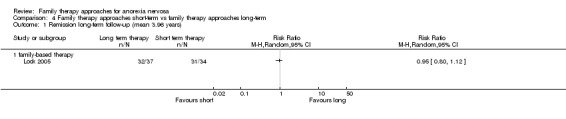
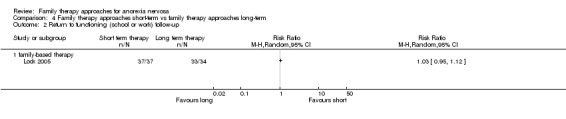
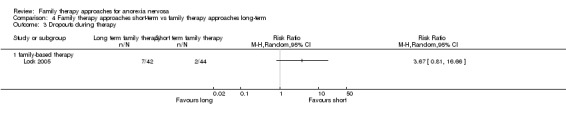
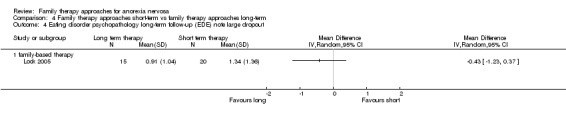
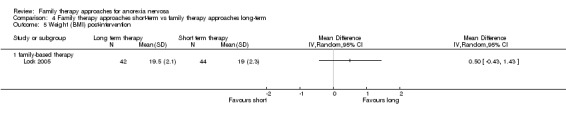
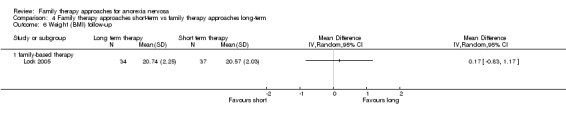
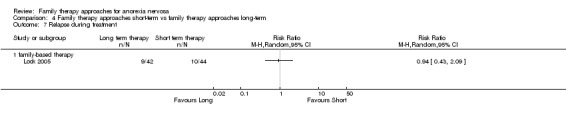
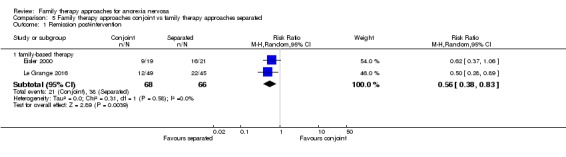
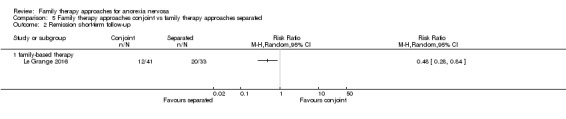
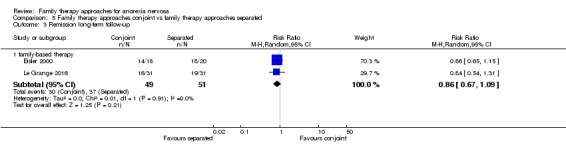
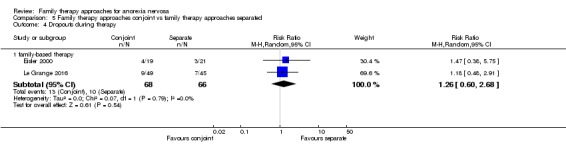
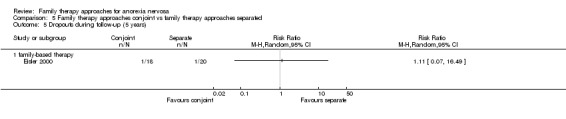
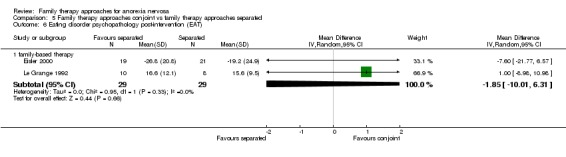
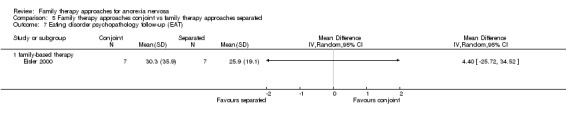
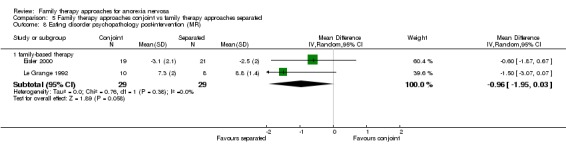
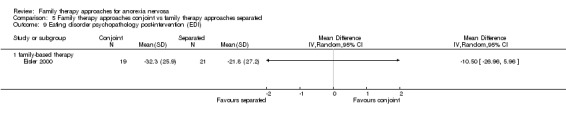
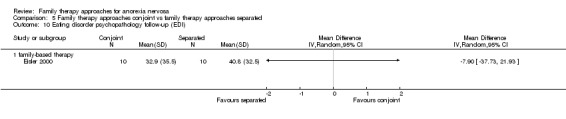
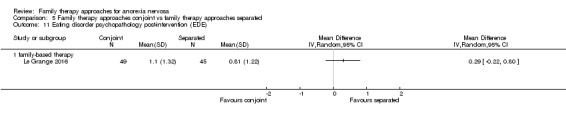
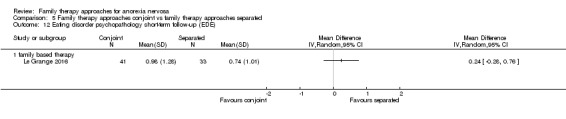
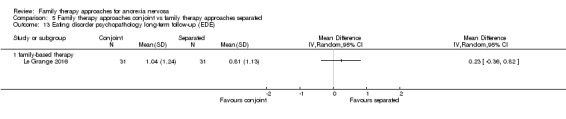
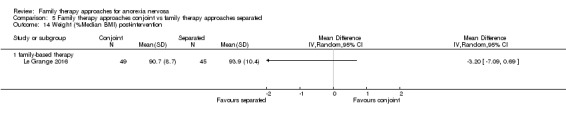
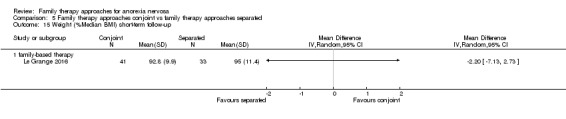
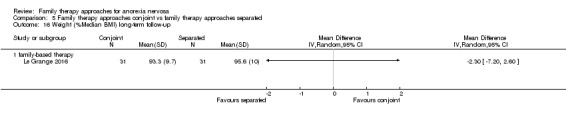
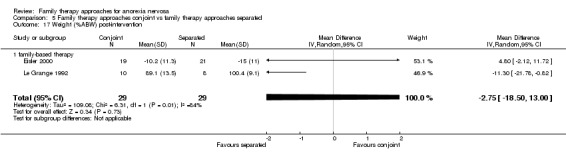
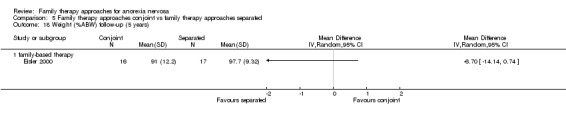
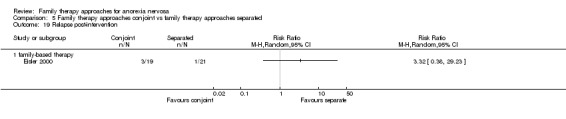
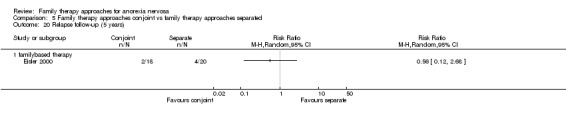
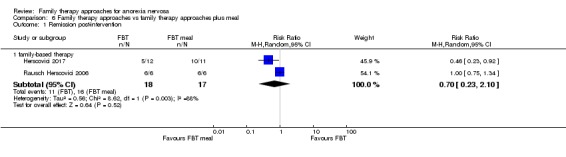
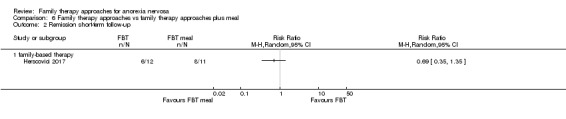
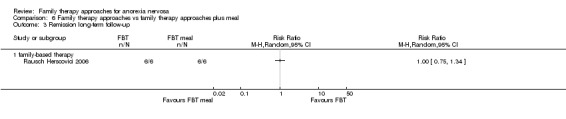
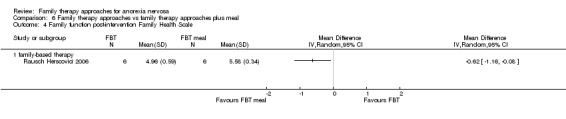
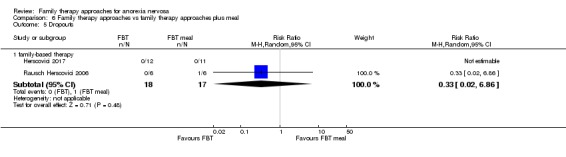
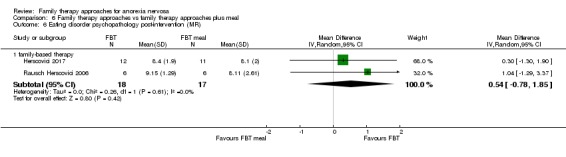
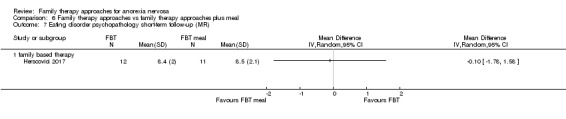
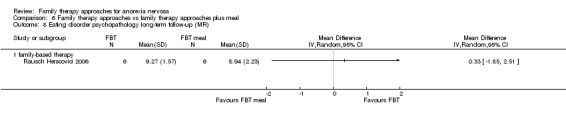
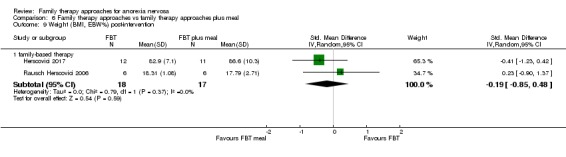
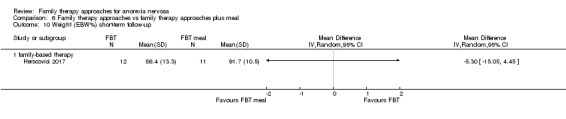
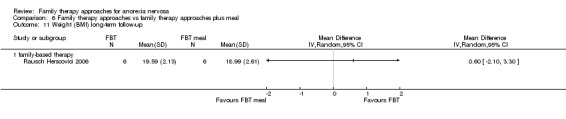
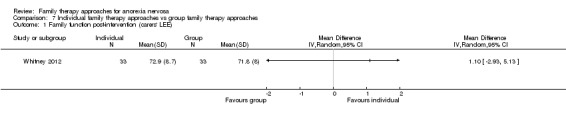
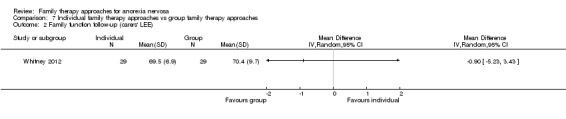
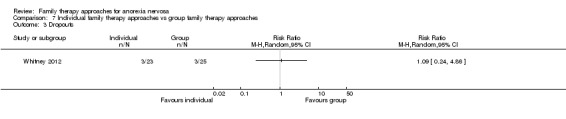
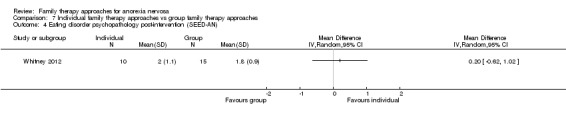
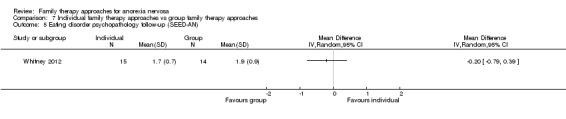
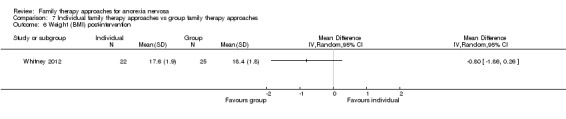
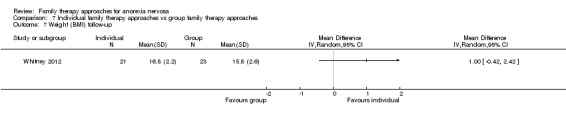
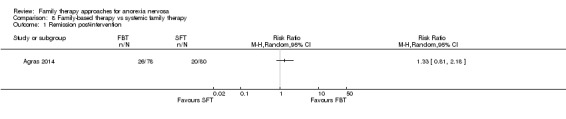
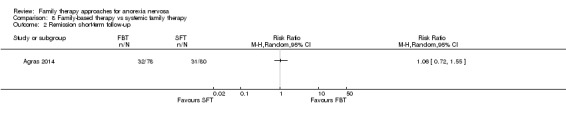
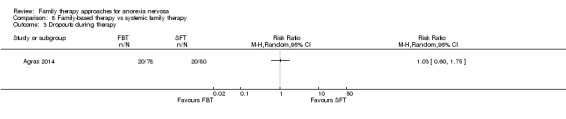
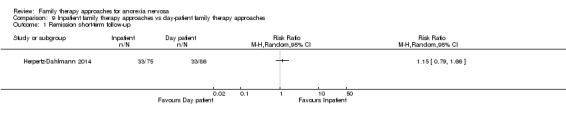
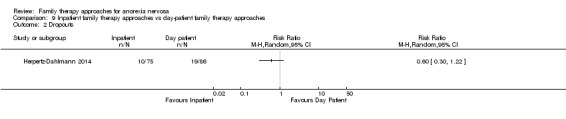
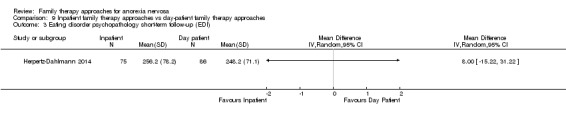
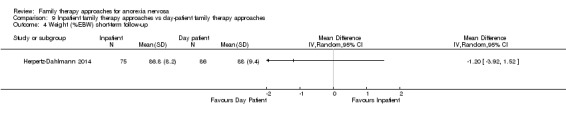
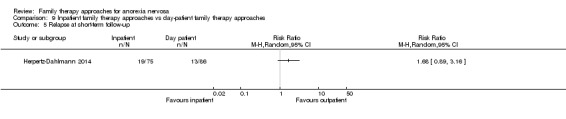
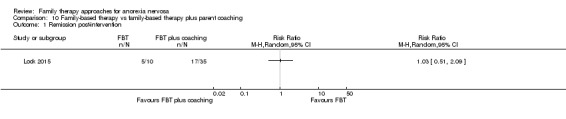
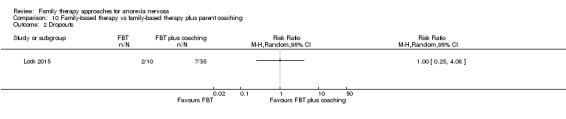
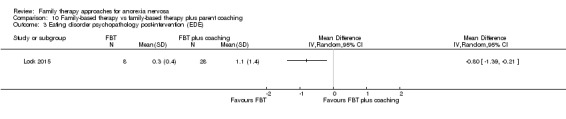
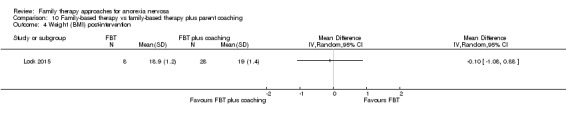
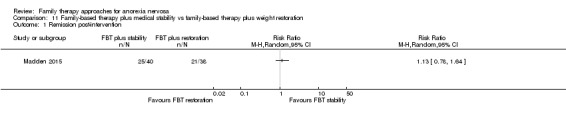
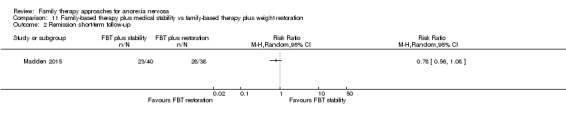
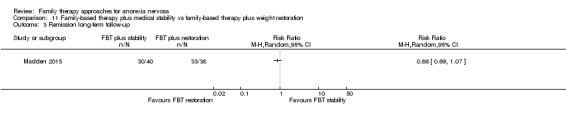
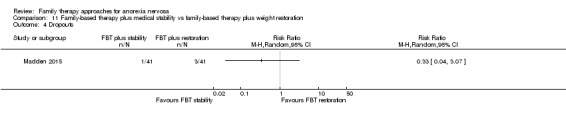
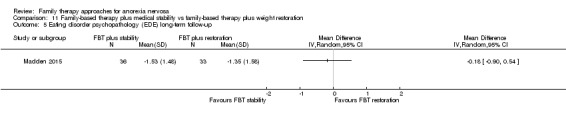
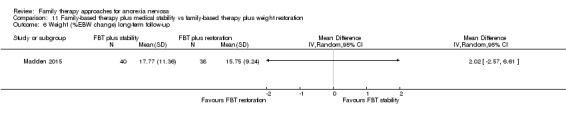
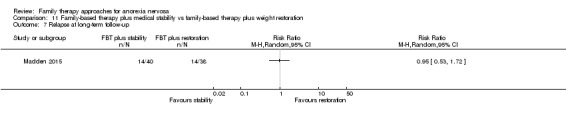
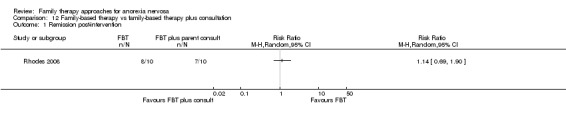
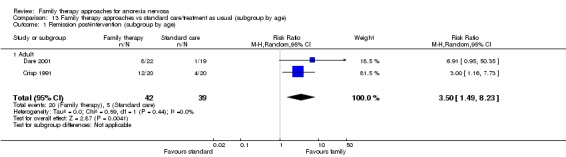
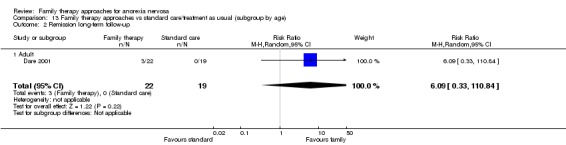
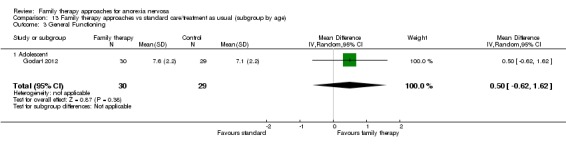
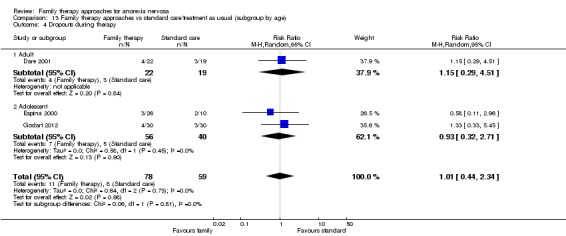
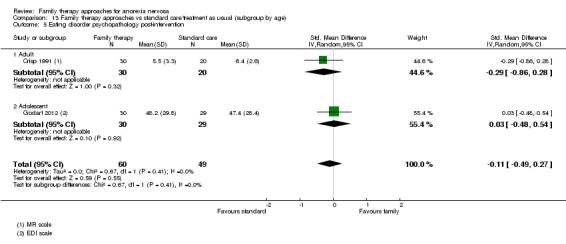
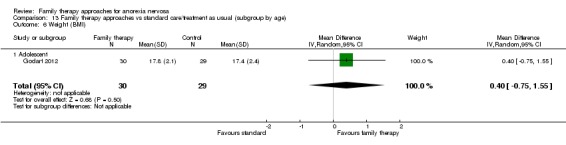
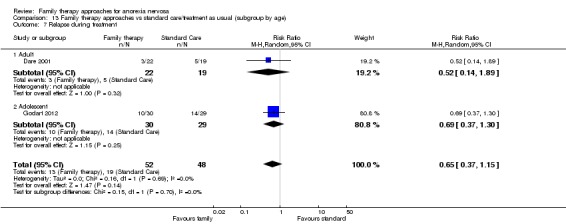
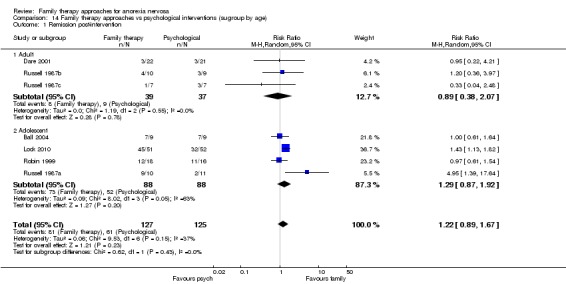
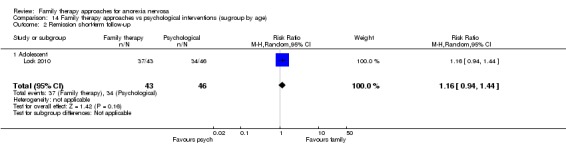
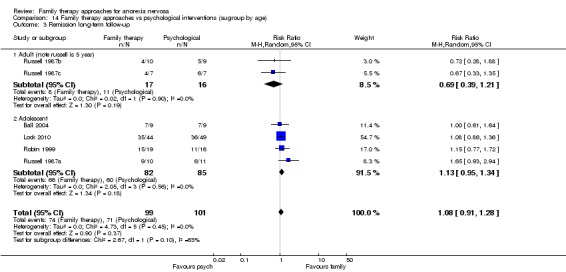
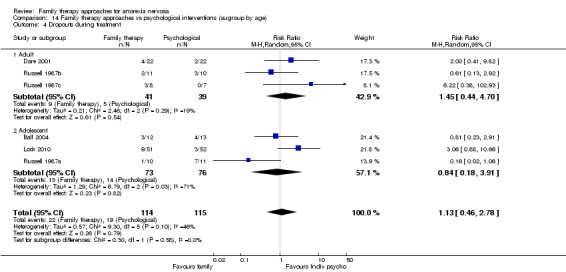
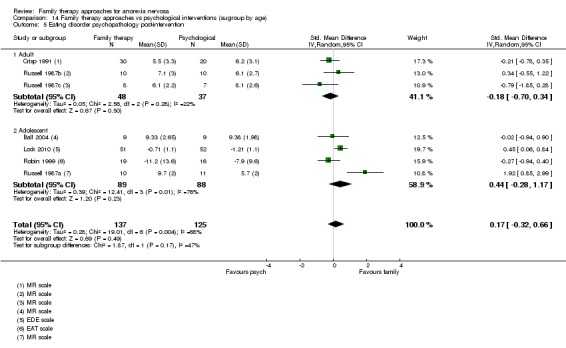
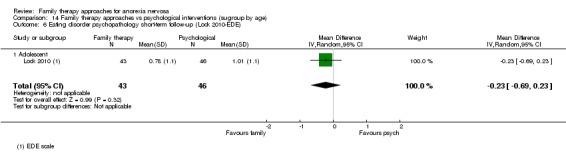
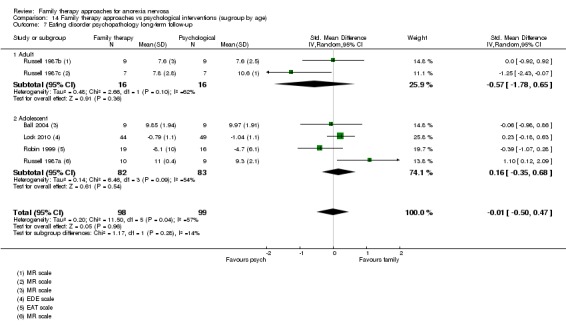
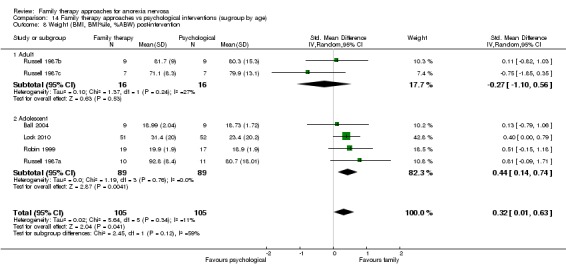
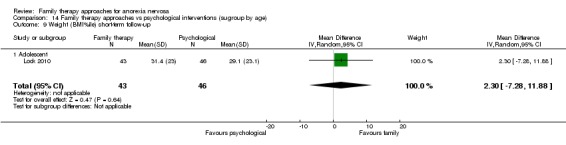
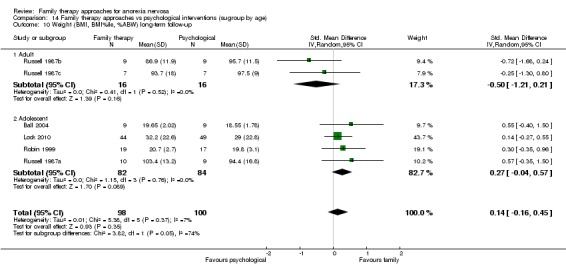
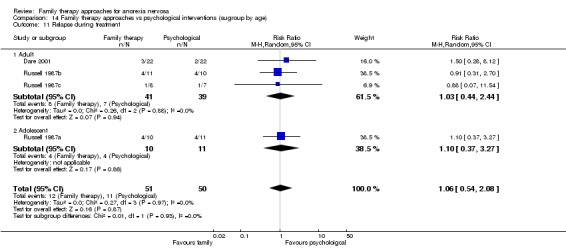
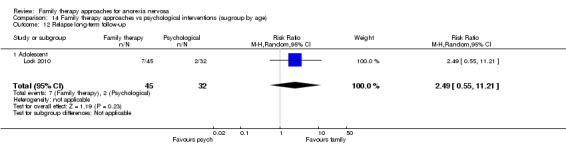
Main results: We included 25 trials in this version of the review (13 from the original 2010 review and 12 newly-included studies). Sixteen trials were of adolescents, eight trials of adults (seven of these in young adults aged up to 26 years) and one trial included three age groups: one adolescent, one young adult and one adult. Most investigated family-based therapy or variants. Reporting of trial conduct was generally inadequate, so that in a large number of studies we rated the risk of bias as unclear for many of the domains. Selective reporting bias was particularly problematic, with 68% of studies rated at high risk of bias in this area, followed by incomplete outcome data, with 44% of studies rated at high risk of bias in this area. For the main outcome measure of remission there was some low-quality evidence (from only two studies, 81 participants) suggesting that family therapy approaches might offer some advantage over treatment as usual on rates of remission, post intervention (risk ratio (RR) 3.50, 95% confidence interval (CI) 1.49 to 8.23; I2 = 0%). However, at follow-up, low-quality evidence from only one study suggested this effect was not maintained. There was very low-quality evidence from only one trial, which means it is difficult to determine whether family therapy approaches offer any advantage over educational interventions for remission (RR 9.00, 95% CI 0.53 to 153.79; 1 study, N = 30). Similarly, there was very low-quality evidence from only five trials for remission post-intervention, again meaning that it is difficult to determine whether there is any advantage of family therapy approaches over psychological interventions (RR 1.22, 95% CI 0.89 to 1.67; participants = 252; studies = 5; I2 = 37%) and at long-term follow-up (RR 1.08, 95% CI 0.91 to 1.28; participants = 200; studies = 4 with 1 of these contributing 3 pairwise comparisons for different age groups; I2 = 0%). There was no indication that the age group had any impact on the overall treatment effect; however, it should be noted that there were very few trials undertaken in adults, with the age range of adult studies included in this analysis from 20 to 27. There was some evidence of a small effect favouring family based therapy compared with other psychological interventions in terms of weight gain post-intervention (standardised mean difference (SMD) 0.32, 95% CI 0.01 to 0.63; participants = 210; studies = 4 with 1 of these contributing 3 pairwise comparisons for different age groups; I2 = 11%) . Overall, there was insufficient evidence to determine whether there were any differences between groups across all comparisons for most of the secondary outcomes (weight, eating disorder psychopathology, dropouts, relapse, or family functioning measures), either at post-intervention or at follow-up.
Authors' conclusions: There is a limited amount of low-quality evidence to suggest that family therapy approaches may be effective compared to treatment as usual in the short term. This finding is based on two trials that included only a small number of participants, and both had issues about potential bias. There is insufficient evidence to determine whether there is an advantage of family therapy approaches in people of any age compared to educational interventions (one study, very low quality) or psychological therapies (five studies, very low quality). Most studies contributing to this finding were undertaken in adolescents and youth. There are clear potential impacts on how family therapy approaches might be delivered to different age groups and further work is required to understand what the resulting effects on treatment efficacy might be. There is insufficient evidence to determine whether one type of family therapy approach is more effective than another. The field would benefit from further large, well-conducted trials.
Conflict of interest statement
Caroline Fisher: None known; Sonja Skocic: None known; Katheleen Rutherford: None known; Sarah Hetrick: None known.
Figures
Update of
-
Family therapy for anorexia nervosa.Cochrane Database Syst Rev. 2010 Apr 14;(4):CD004780. doi: 10.1002/14651858.CD004780.pub2. Cochrane Database Syst Rev. 2010. Update in: Cochrane Database Syst Rev. 2018 Oct 15;10:CD004780. doi: 10.1002/14651858.CD004780.pub3. PMID: 20393940 Updated.
References
References to studies included in this review
-
- Agras WS. Family therapy in the treatment of adolescent anorexia nervosa. NIH CRISP. [CRSREF: 2855946; NIH grant number: 5U01MH076290]
- Agras WS, Lock J, Brandt H, Bryson SW, Dodge E, Halmi KA, et al. Comparison of 2 family therapies for adolescent anorexia nervosa: a randomized parallel trial. JAMA Psychiatry 2014;71(11):1279‐86. [DOI: :10.1001/jamapsychiatry.2014.1025] - PMC - PubMed
- Lock J, Agras WS, Bryson SW, Brandt H, Halmi KA, Kaye W, et al. Does family‐based treatment reduce the need for hospitalization in adolescent anorexia nervosa?. International Journal of Eating Disorders 2016;49(9):891–4. [DOI: 10.1002/eat.22536] - DOI - PubMed
- Lock J, Brandt H, Woodside B, Agras S, Halmi WK, Johnson C, et al. Challenges in conducting a multi‐site randomized clinical trial comparing treatments for adolescent anorexia nervosa. International Journal of Eating Disorders 2012;45(2):202‐13. [DOI: 10.1002/eat.20923] - DOI - PMC - PubMed
- Sadeh‐Sharvit S, Arnow KD, Osipov L, Lock JD, Jo B, Pajarito S, et al. Are parental self‐efficacy and family flexibility mediators of treatment for anorexia nervosa?. International Journal of Eating Disorders 2018;51(3):275‐80. - PMC - PubMed
-
- Ball J, Mitchell P. A randomized controlled study of cognitive behaviour therapy and behavioral family therapy for anorexia nervosa patients. Eating Disorders 2004;12(4):303‐14. - PubMed
- Ball JR. A controlled evaluation of psychological treatments for anorexia nervosa. (cognitive behavior therapy, behavioral family therapy). Dissertation Abstracts International 1999;59(11‐B):5781.
- Ball JR, Mitchell PB, Touyz SW, Griffiths RA, Beumont PJ. Clinical utility of the modified Stroop task as a treatment outcome measure: Questions raised. Clinical Psychologist 2004;8(2):76‐80.
-
- Besharat MA. The predictive value of family expressed emotion in eating disorders. Iranian Journal of Medical Sciencse 2001;26(3 & 4):110‐5.
-
- Crisp AH, Norton K, Gowers S, Halek C, Bowyer C, Yeldham D, et al. A controlled study of the effect of therapies aimed at adolescent and family psychopathology in anorexia nervosa. British Journal of Psychiatry 1991;159:325‐33. - PubMed
- Gowers S, Norton K, Halek C, Crisp AH. Outcome of outpatient psychotherapy in a random allocation treatment study of anorexia nervosa. International Journal of Eating Disorders 1994;15(2):165‐77. - PubMed
- Gowers S, Phil M, Norton K, Yeldham D, Bowyer C, Levett G, et al. The St. George's prospective treatment study of anorexia nervosa: A discussion of methodological problems. International Journal of Eating Disorders 1989;8(4):445‐54.
-
- Dare C, Eisler I, Russell G, Treasure J, Dodge L. Psychological therapies for adults with anorexia nervosa: Randomised controlled trial of out‐patient treatments. British Journal of Psychiatry 2001;178(3):216‐21. - PubMed
References to studies excluded from this review
-
- Attia E. In the Clinic. Eating disorders. Annals of Internal Medicine 2012;156(7):1‐16. - PubMed
-
- Buddeberg B, Buddeberg C. Family therapy of anorexia nervosa. Praxis der Kinderpsychologie und Kinderpsychiatrie 1979;28(2):37‐43. - PubMed
-
- Dalle Grave R. Inpatient cognitive behavior therapy for severe eating disorders. Psychological Topics 2010;19(2):323‐40.
-
- Fettes PA, Peters JM. A meta‐analysis of group treatments for bulimia nervosa. International Journal of Eating Disorders 1992;11(2):97‐110.
References to studies awaiting assessment
-
- Bulik C. UCAN: Uniting Couples in the Treatment of Anorexia Nervosa (UCAN). clinicaltrials.gov/ct2/show/NCT00928109 (first received 25 June 2009). - PMC - PubMed
-
- Dimitropoulos G. Multi‐family group therapy for adult eating disorders (MFGT). clinicaltrials.gov/show/NCT02106728 (first received 8 April 2014).
-
- Eisler I. A multi‐centre randomised trial of the outcome, acceptability and cost‐effectiveness of family therapy and multi‐family day treatment compared with inpatient care and outpatient family therapy for adolescent anorexia nervosa. www.isrctn.com/ISRCTN11275465 (first received 5 April 2006).
- Eisler I, Simic M, Hodsoll J, Asen E, Berelowitz M, Connan F, et al. A pragmatic randomised multi‐centre trial of multifamily and single family therapy for adolescent anorexia nervosa. BMC Psychiatry 2016;16(1):422. - PMC - PubMed
-
- Gore‐Rees, P. A randomised controlled multicentre treatment of adolescent anorexia nervosa including assessment of cost and patient acceptability. National Research Register [Archived]. - PubMed
-
- Jacobi C. Early detection and intervention of anorexia nervosa in adolescent girls: a randomized controlled trial comparing a family‐oriented, internet‐based intervention with a control group without intervention. www.isrctn.com/ISRCTN18614564 (first received 6 January 2012).
References to ongoing studies
-
- Bilyk BF. Effectiveness of a cognitive behavioral management pilot program in a sample of Brazilian adolescents with anorexia vervosa [Efetividade de um programa piloto de tratamento cognitivo comportamental em uma amostra de adolescentes brasileiros com anorexia nervosa]. www.ensaiosclinicos.gov.br/rg/RBR‐4dpths/ (first received 14 September 2017). [Trial ID: U1111‐1202‐0493]
-
- Bulik C, Baucom D. UNCAN2: Enhancing treatment for adult anorexia with a couple‐based approach. clinicaltrials.gov/show/NCT01740752 (first received 4 December 2012).
-
- Carrot B. Family therapy and anorexia nervosa : Which is the best approach? (THERAFAMBEST). clinicaltrials.gov/ct2/show/NCT03350594 (first received 22 November 2017).
-
- Hildebrandt T. Reward systems and food avoidance in eating disorders. clinicaltrials.gov/ct2/show/NCT02795455 (first received 10 June 2016).
-
- Lock JD. Adaptive treatment for adolescent anorexia nervosa. clinicaltrials.gov/ct2/show/NCT03097874 (first received 31 March 2017).
Additional references
-
- Achenbach T. Manual for the Youth Self‐Report and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry, 1991.
-
- Angold A, Costello EJ, Messer SC, Pickles A. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research 1995;5(4):237‐249.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM‐IV). 4th Edition. Washington, DC: American Psychiatric Association, 1994.
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM‐5. 5th Edition. Washington, D.C.: American Psychiatric Association, 2013. [APA (2013); APA, 2013]
-
- Back EA. Effects of parental relations and upbringing in troubled adolescent eating behaviors. Eating Disorders 2011;19:403‐24. - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous