

Supratotal resection in glioma: a systematic review
- PMID: 30321384
- PMCID: PMC6374756
- DOI: 10.1093/neuonc/noy166
Supratotal resection in glioma: a systematic review
Abstract
Background: Emerging evidence suggests survival benefit from resection beyond all MRI abnormalities present on T1-enhanced and T2‒fluid attenuated inversion recovery (FLAIR) modalities in glioma (supratotal resection); however, the quality of evidence is unclear. We addressed this question via systematic review of the literature.
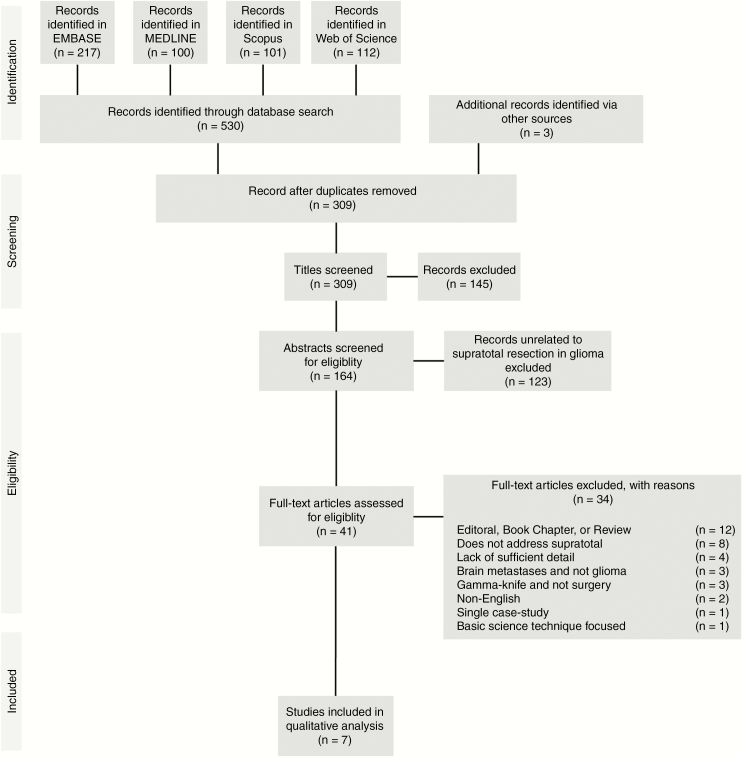
Methods: EMBASE, MEDLINE, Scopus, and Web of Science databases were queried. Case studies, reviews or editorials, non-English, abstract-only, brain metastases, and descriptive works were excluded. All others were included.
Results: Three hundred and nine unique references yielded 41 studies for full-text review, with 7 included in the final analysis. Studies were mostly of Oxford Center for Evidence-Based Medicine Level 4 quality. A total of 88 patients underwent supratotal resection in a combined cohort of 492 patients (214 males and 278 females, age 18 to 82 years). Fifty-one supratotal resections were conducted on high-grade gliomas, and 37 on low-grade gliomas. Karnofsky performance status, overall survival, progression-free survival, neurological deficits postoperatively, and anaplastic transformation were the main measured outcomes. No randomized controlled trials were identified. Preliminary low-quality support was found for supratotal resection in increasing overall survival and progression-free survival for both low-grade and high-grade glioma.
Conclusion: The literature suggests insufficient evidence for carte blanche application of supratotal resection, particularly in lower-grade gliomas where neurological deficits can result in long-term disability. While the preliminary studies discussed here, containing data from only a few centers, have reported increased progression-free and overall survival, these claims require validation in prospective research studies involving larger patient populations with clearly defined appropriate outcome metrics in order to reduce potential bias.
Keywords: FLAIR; glioma; resection; supratotal; surgery.
© The Author(s) 2018. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Ricard D, Idbaih A, Ducray F, Lahutte M, Hoang-Xuan K, Delattre JY. Primary brain tumours in adults. Lancet. 2012;379(9830):1984–1996. - PubMed
-
- Mandonnet E, Delattre JY, Tanguy ML, et al. . Continuous growth of mean tumor diameter in a subset of grade II gliomas. Ann Neurol. 2003;53(4):524–528. - PubMed
-
- Brandes AA, Tosoni A, Franceschi E, Reni M, Gatta G, Vecht C. Glioblastoma in adults. Crit Rev Oncol Hematol. 2008;67(2):139–152. - PubMed
-
- Miranda A, Blanco-Prieto M, Sousa J, Pais A, Vitorino C. Breaching barriers in glioblastoma. Part I: molecular pathways and novel treatment approaches. Int J Pharm. 2017;531(1):372–388. - PubMed
-
- Bush NA, Chang SM, Berger MS. Current and future strategies for treatment of glioma. Neurosurg Rev. 2017;40(1):1–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
