

Baseline metabolic profiles of early rheumatoid arthritis patients achieving sustained drug-free remission after initiating treat-to-target tocilizumab, methotrexate, or the combination: insights from systems biology
- PMID: 30322408
- PMCID: PMC6235217
- DOI: 10.1186/s13075-018-1729-2
Baseline metabolic profiles of early rheumatoid arthritis patients achieving sustained drug-free remission after initiating treat-to-target tocilizumab, methotrexate, or the combination: insights from systems biology
Abstract
Background: We previously identified, in newly diagnosed rheumatoid arthritis (RA) patients, networks of co-expressed genes and proteomic biomarkers associated with achieving sustained drug-free remission (sDFR) after treatment with tocilizumab- or methotrexate-based strategies. The aim of this study was to identify, within the same patients, metabolic pathways important for achieving sDFR and to subsequently study the complex interactions between different components of the biological system and how these interactions might affect the therapeutic response in early RA.
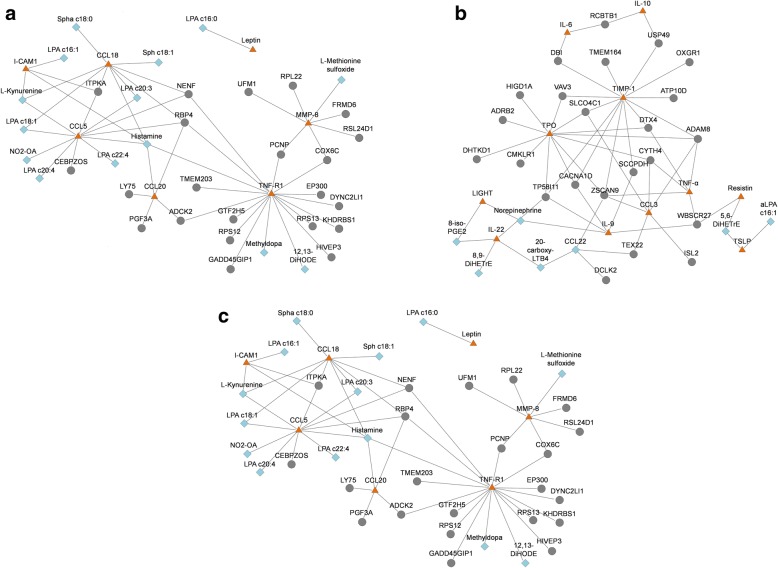
Methods: Serum samples were analyzed of 60 patients who participated in the U-Act-Early trial (ClinicalTrials.gov number NCT01034137) and initiated treatment with methotrexate, tocilizumab, or the combination and who were thereafter able to achieve sDFR (n = 37); as controls, patients were selected who never achieved a drug-free status (n = 23). Metabolomic measurements were performed using mass spectrometry on oxidative stress, amine, and oxylipin platforms covering various compounds. Partial least square discriminant analyses (PLSDA) were performed to identify, per strategy arm, relevant metabolites of which the biological pathways were studied. In addition, integrative analyses were performed correlating the previously identified transcripts and proteins with the relevant metabolites.
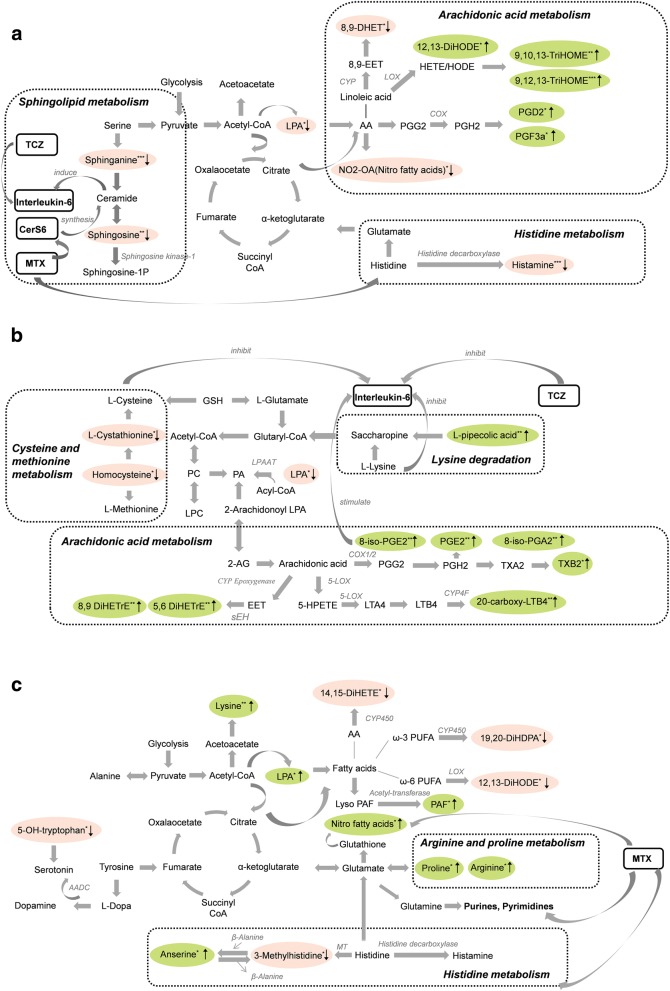
Results: In the tocilizumab plus methotrexate, tocilizumab, and methotrexate strategy, respectively, 19, 13, and 12 relevant metabolites were found, which were subsequently used for pathway analyses. The most significant pathway in the tocilizumab plus methotrexate strategy was "histidine metabolism" (p < 0.001); in the tocilizumab strategy it was "arachidonic acid metabolism" (p = 0.018); and in the methotrexate strategy it was "arginine and proline metabolism" (p = 0.022). These pathways have treatment-specific drug interactions with metabolites affecting either the signaling of interleukin-6, which is inhibited by tocilizumab, or affecting protein synthesis from amino acids, which is inhibited by methotrexate.
Conclusion: In early RA patients treated-to-target with a tocilizumab- or methotrexate-based strategy, several metabolites were found to be associated with achieving sDFR. In line with our previous observations, by analyzing relevant transcripts and proteins within the same patients, the metabolic profiles were found to be different between the strategy arms. Our metabolic analysis further supports the hypothesis that achieving sDFR is not only dependent on predisposing biomarkers, but also on the specific treatment that has been initiated.
Trial registration: ClinicalTrials.gov, NCT01034137 . Registered on January 2010.
Keywords: Drug-free remission; Metabolomics; Methotrexate; Rheumatoid arthritis; Tocilizumab.
Conflict of interest statement
Ethics approval and consent to participate
The medical ethics research committee of the University Medical Center Utrecht approved the study for all participating hospitals. All patients signed informed consent before study entry.
Consent for publication
Not applicable.
Competing interests
The department of the authors who included patients (JWGJ and JWJB) in the U-Act-Early trial received reimbursements from Roche Nederland BV. JWJB reported grants and fees from Roche, AbbVie, Bristol-Myers Squibb, Merck Sharp & Dohme, Pfizer, and UCB. JMvL received fees from Arthrogen, MSD, Pfizer, Eli Lilly, and BMS and research grants from Astra Zeneca, Roche-Genentech. FPJGL reports grants from Roche. AP-S is an employee of F Hoffmann-La Roche and MEAB is an employee of Roche Nederland BV. XMT, WY, ACH, and TH declare no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Can metabolomic profiling predict response to therapy?Nat Rev Rheumatol. 2019 Mar;15(3):129-130. doi: 10.1038/s41584-018-0136-z. Nat Rev Rheumatol. 2019. PMID: 30531855 No abstract available.
References
-
- Stolt P, Bengtsson C, Nordmark B, Lindblad S, Lundberg I, Klareskog L, Alfredsson L, EIRA study group Quantification of the influence of cigarette smoking on rheumatoid arthritis: results from a population based case-control study, using incident cases. Ann Rheum Dis. 2003;62(9):835–841. doi: 10.1136/ard.62.9.835. - DOI - PMC - PubMed
-
- van Nies JA, Tsonaka R, Gaujoux-Viala C, Fautrel B, van der Helm-van Mil AH. Evaluating relationships between symptom duration and persistence of rheumatoid arthritis: does a window of opportunity exist? Results on the Leiden early arthritis clinic and ESPOIR cohorts. Ann Rheum Dis. 2015;74(5):806–812. doi: 10.1136/annrheumdis-2014-206047. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
