

Single cell RNA-seq reveals profound transcriptional similarity between Barrett's oesophagus and oesophageal submucosal glands
- PMID: 30323168
- PMCID: PMC6189174
- DOI: 10.1038/s41467-018-06796-9
Single cell RNA-seq reveals profound transcriptional similarity between Barrett's oesophagus and oesophageal submucosal glands
Abstract
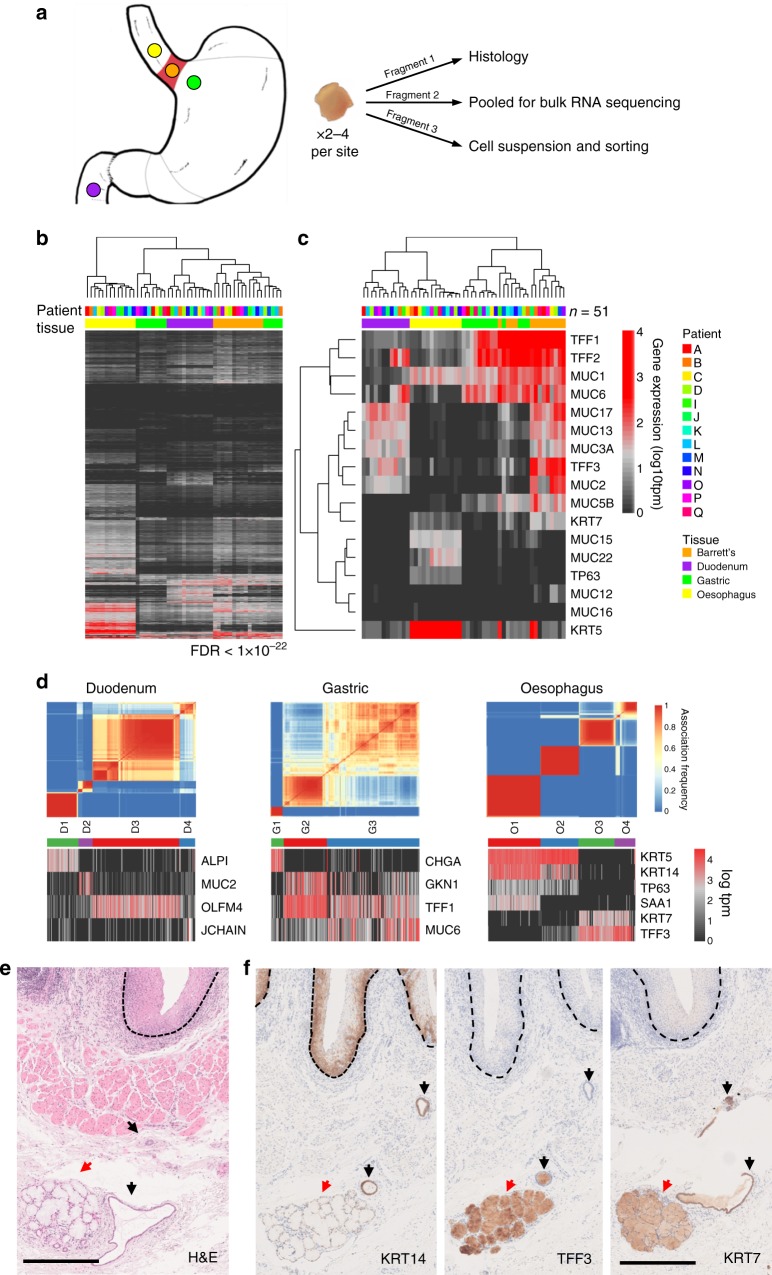
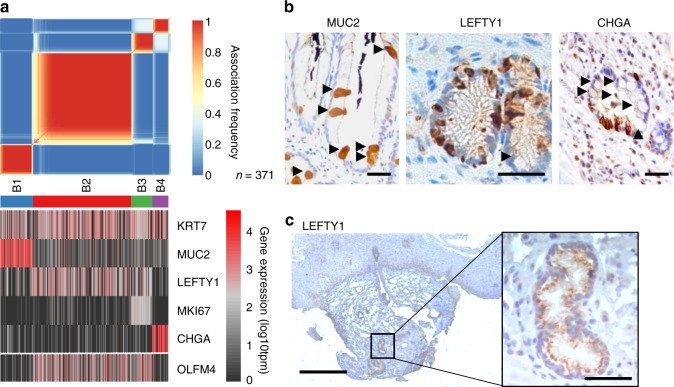
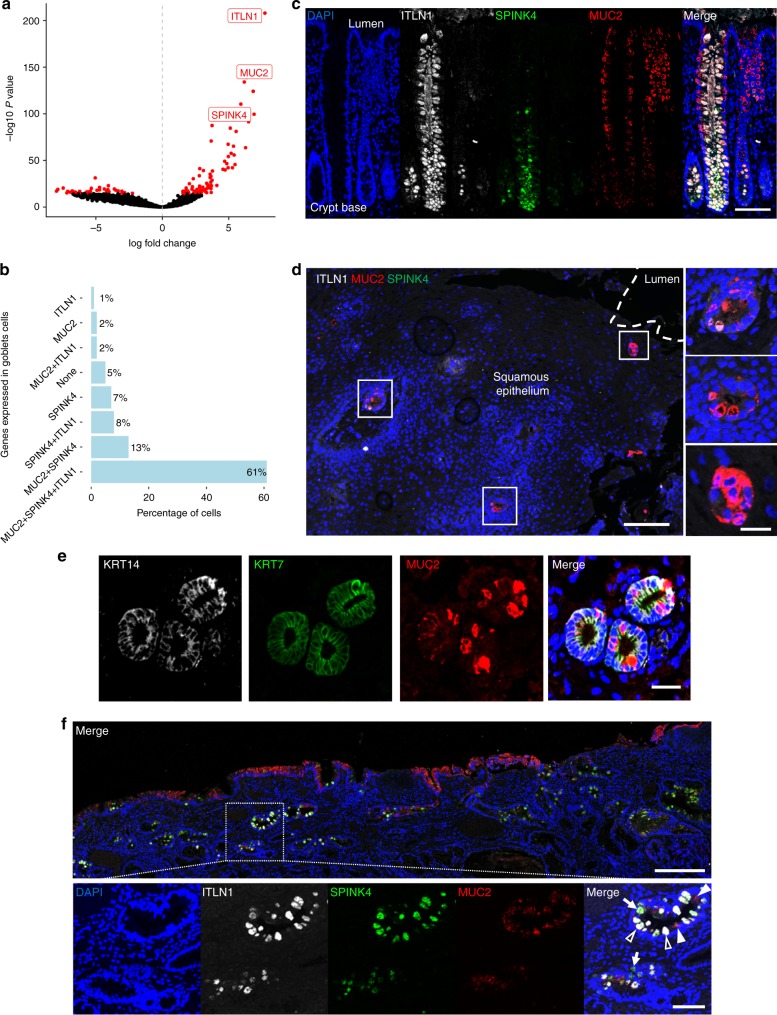
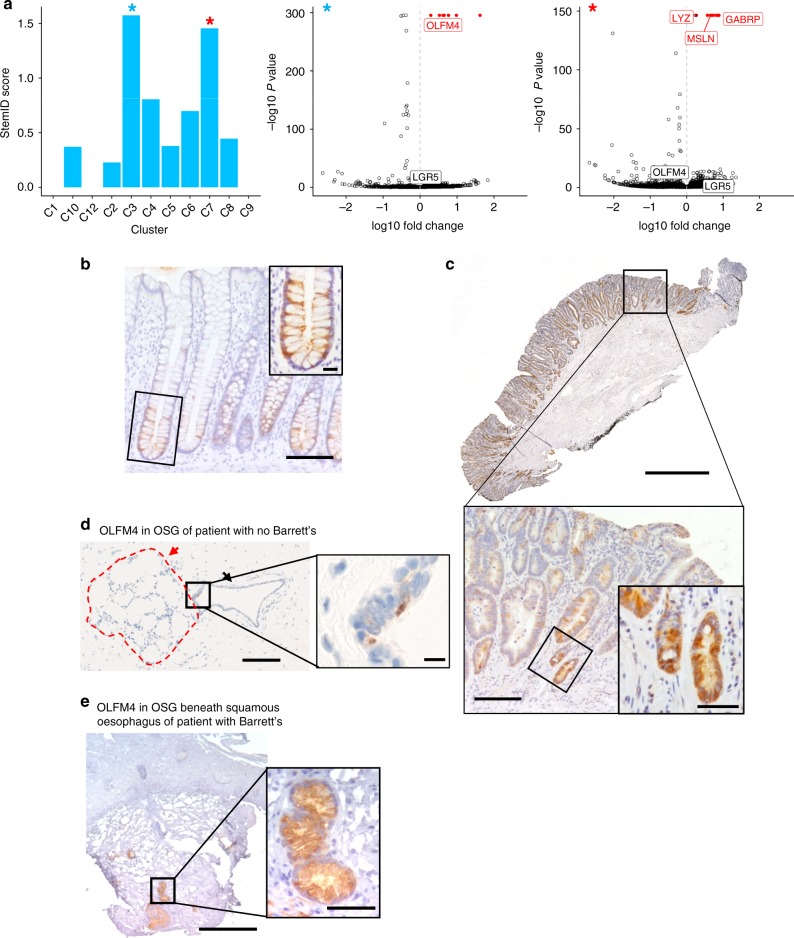
Barrett's oesophagus is a precursor of oesophageal adenocarcinoma. In this common condition, squamous epithelium in the oesophagus is replaced by columnar epithelium in response to acid reflux. Barrett's oesophagus is highly heterogeneous and its relationships to normal tissues are unclear. Here we investigate the cellular complexity of Barrett's oesophagus and the upper gastrointestinal tract using RNA-sequencing of single cells from multiple biopsies from six patients with Barrett's oesophagus and two patients without oesophageal pathology. We find that cell populations in Barrett's oesophagus, marked by LEFTY1 and OLFM4, exhibit a profound transcriptional overlap with oesophageal submucosal gland cells, but not with gastric or duodenal cells. Additionally, SPINK4 and ITLN1 mark cells that precede morphologically identifiable goblet cells in colon and Barrett's oesophagus, potentially aiding the identification of metaplasia. Our findings reveal striking transcriptional relationships between normal tissue populations and cells in a premalignant condition, with implications for clinical practice.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Cancer Research UK. http://www.cancerresearchuk.org/health-professional/cancer-statistics/st... (2016).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
