

Neuroimaging of Sleep Disturbances in Movement Disorders
- PMID: 30323786
- PMCID: PMC6141751
- DOI: 10.3389/fneur.2018.00767
Neuroimaging of Sleep Disturbances in Movement Disorders
Abstract
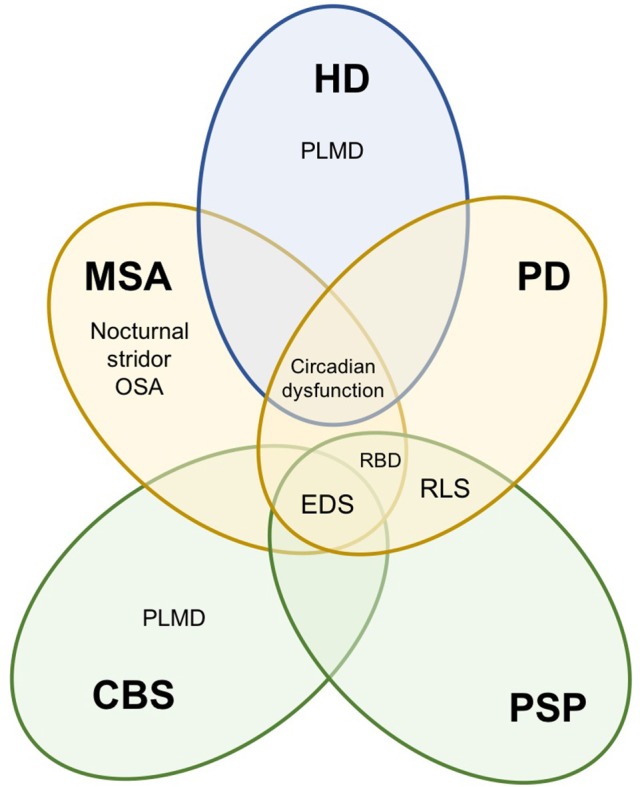
Sleep dysfunction is recognized as a distinct clinical manifestation in movement disorders, often reported early on in the disease course. Excessive daytime sleepiness, rapid eye movement sleep behavior disorder and restless leg syndrome, amidst several others, are common sleep disturbances that often result in significant morbidity. In this article, we review the spectrum of sleep abnormalities across atypical Parkinsonian disorders including multiple system atrophy (MSA), progressive supranuclear palsy (PSP) and corticobasal syndrome (CBS), as well as Parkinson's disease (PD) and Huntington's disease (HD). We also explore the current concepts on the neurobiological underpinnings of sleep disorders, including the role of dopaminergic and non-dopaminergic pathways, by evaluating the molecular, structural and functional neuroimaging evidence based on several novel techniques including magnetic resonance imaging (MRI), functional magnetic resonance imaging (fMRI), diffusion tensor imaging (DTI), single-photon emission computed tomography (SPECT) and positron emission tomography (PET). Based on the current state of research, we suggest that neuroimaging is an invaluable tool for assessing structural and functional correlates of sleep disturbances, harboring the ability to shed light on the sleep problems attached to the limited treatment options available today. As our understanding of the pathophysiology of sleep and wake disruption heightens, novel therapeutic approaches are certain to transpire.
Keywords: Parkinson's disease; REM behavior sleep disorder; atypical Parkinsonism; excessive daytime sleepiness; magnetic resonance imaging; neuroimaging; positron emission tomography; sleep.
Figures
Similar articles
-
Sleep disturbances in progressive supranuclear palsy syndrome (PSPS) and corticobasal syndrome (CBS).Neurol Neurochir Pol. 2023;57(3):229-234. doi: 10.5603/PJNNS.a2023.0019. Epub 2023 Mar 17. Neurol Neurochir Pol. 2023. PMID: 36928793 Review.
-
Neuroimaging Advances in Parkinson's Disease and Atypical Parkinsonian Syndromes.Front Neurol. 2020 Oct 15;11:572976. doi: 10.3389/fneur.2020.572976. eCollection 2020. Front Neurol. 2020. PMID: 33178113 Free PMC article. Review.
-
Overview of sleep disturbances and their management in Parkinson plus disorders.J Neurol Sci. 2020 Aug 15;415:116891. doi: 10.1016/j.jns.2020.116891. Epub 2020 May 8. J Neurol Sci. 2020. PMID: 32446010 Review.
-
Sleep disturbances and brain MRI morphometry in Parkinson's disease, multiple system atrophy and progressive supranuclear palsy - a comparative study.Parkinsonism Relat Disord. 2010 May;16(4):275-9. doi: 10.1016/j.parkreldis.2010.01.002. Epub 2010 Feb 24. Parkinsonism Relat Disord. 2010. PMID: 20185356
-
Differentiation of progressive supranuclear palsy: clinical, imaging and laboratory tools.Acta Neurol Scand. 2013 May;127(5):362-70. doi: 10.1111/ane.12067. Epub 2013 Feb 13. Acta Neurol Scand. 2013. PMID: 23406296 Review.
Cited by
-
Striatum Shape Hypertrophy in Early Stage Parkinson's Disease With Excessive Daytime Sleepiness.Front Neurosci. 2020 Jan 9;13:1353. doi: 10.3389/fnins.2019.01353. eCollection 2019. Front Neurosci. 2020. PMID: 31992965 Free PMC article.
-
White Matter Tract Alterations in Drug-Naïve Parkinson's Disease Patients With Excessive Daytime Sleepiness.Front Neurol. 2019 Apr 16;10:378. doi: 10.3389/fneur.2019.00378. eCollection 2019. Front Neurol. 2019. PMID: 31057475 Free PMC article.
-
Diffusion Tensor Imaging Reveals Deep Brain Structure Changes in Early Parkinson's Disease Patients with Various Sleep Disorders.Brain Sci. 2022 Mar 30;12(4):463. doi: 10.3390/brainsci12040463. Brain Sci. 2022. PMID: 35447994 Free PMC article.
-
Recent Progress in Non-motor Features of Parkinson's Disease with a Focus on Circadian Rhythm Dysregulation.Neurosci Bull. 2021 Jul;37(7):1010-1024. doi: 10.1007/s12264-021-00711-x. Epub 2021 Jun 15. Neurosci Bull. 2021. PMID: 34128188 Free PMC article. Review.
-
VMAT2 availability in Parkinson's disease with probable REM sleep behaviour disorder.Mol Brain. 2021 Nov 10;14(1):165. doi: 10.1186/s13041-021-00875-7. Mol Brain. 2021. PMID: 34758845 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous