

Prevalence of and reasons for women's, family members', and health professionals' preferences for cesarean section in China: A mixed-methods systematic review
- PMID: 30325928
- PMCID: PMC6191094
- DOI: 10.1371/journal.pmed.1002672
Prevalence of and reasons for women's, family members', and health professionals' preferences for cesarean section in China: A mixed-methods systematic review
Abstract
Background: China has witnessed a rapid increase of cesarean section (CS) rates in recent years. Several non-clinical factors have been cited as contributing to this trend including maternal request and perceived convenience. We aimed to assess preferences for mode of delivery and reasons for preferences for CS in China to inform the development of future interventions to mitigate unnecessary CSs, which are those performed in the absence of medical indications.
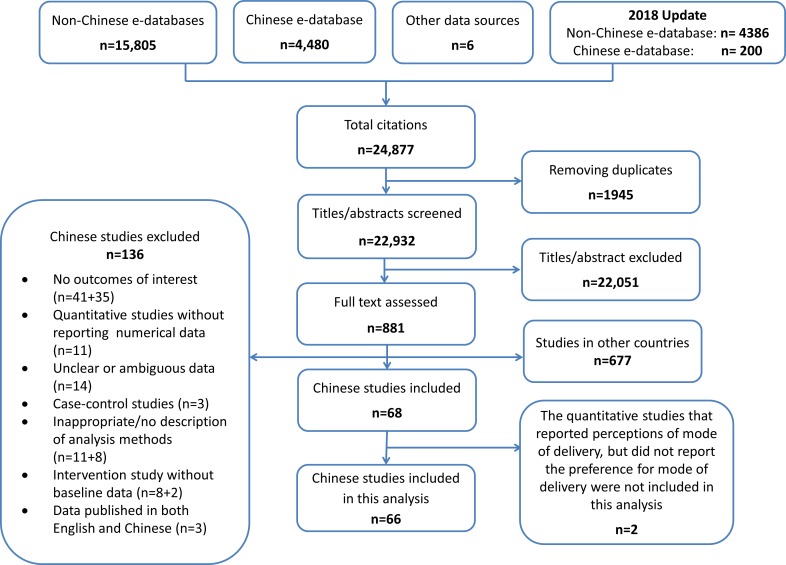
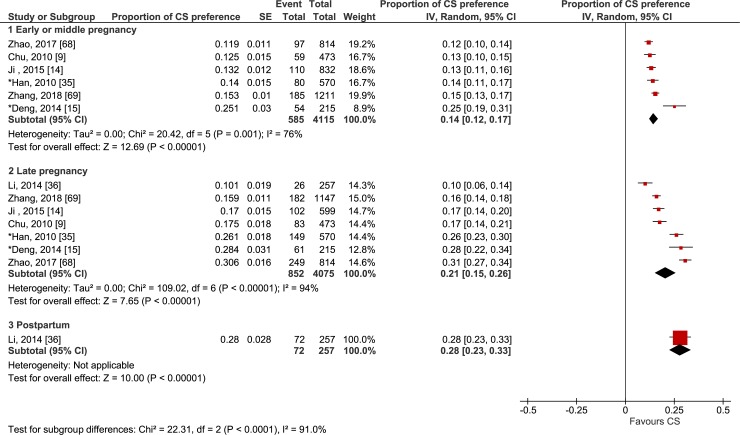
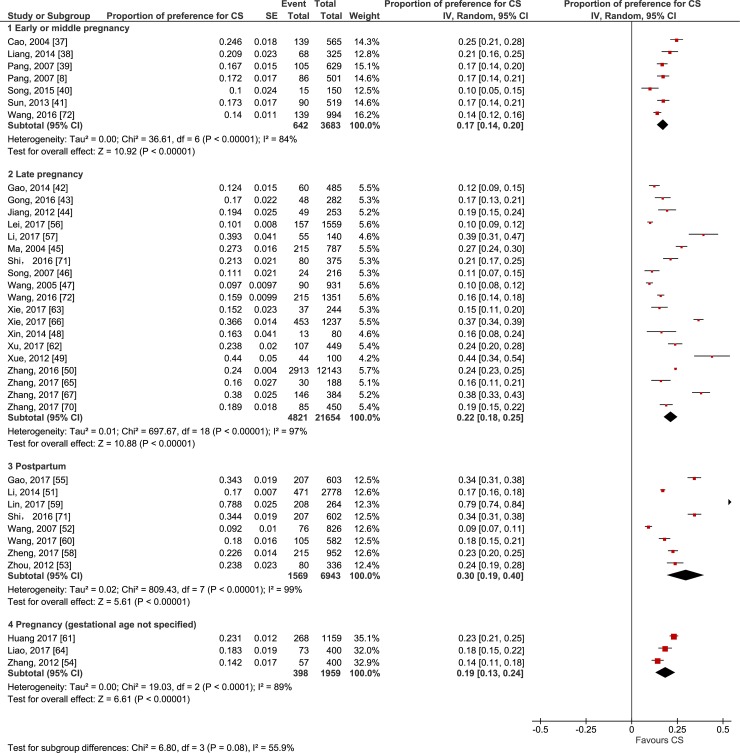
Methods and findings: We conducted a mixed-methods systematic review and included longitudinal, cross-sectional, and qualitative studies in mainland China, Hong Kong, and Taiwan that investigated preferences for mode of delivery among women and family members and health professionals, and the reasons underlying such preferences. We searched MEDLINE/PubMed, Embase, CINAHL, POPLINE, PsycINFO, Global Health Library, and one Chinese database (CNKI) using a combination of the key terms 'caesarean section', 'preference', 'choice', 'knowledge', 'attitude', 'culture', 'non-clinical factors', and 'health professionals-patient relations' between 1990 and 2018 without language restriction. Meta-analysis of quantitative studies and meta-synthesis of qualitative studies were applied. We included 66 studies in this analysis: 47 quantitative and 19 qualitative. For the index pregnancy, the pooled proportions of preference for CS reported by women in longitudinal studies were 14% in early or middle pregnancy (95% CI 12%-17%) and 21% in late pregnancy (95% CI 15%-26%). In cross-sectional studies, the proportions were 17% in early or middle pregnancy (95% CI 14%-20%), 22% in late pregnancy (95% CI 18%-25%), and 30% postpartum (95% CI 19%-40%). Women's preferences for CS were found to rise as pregnancy progressed (preference change across longitudinal studies: mean difference 7%, 95% CI 1%-13%). One longitudinal study reported that the preference for CS among women's partners increased from 8% in late pregnancy to 17% in the immediate postpartum period. In addition, 18 quantitative studies revealed that some pregnant women, ranging from 4% to 34%, did not have a straightforward preference for a mode of delivery, even in late pregnancy. The qualitative meta-synthesis found that women's perceptions of CS as preferable were based on prioritising the baby's and woman's health and appeared to intensify through interactions with the health system. Women valued the convenience of bypassing labour because of fear of pain, antagonistic relations with providers, and beliefs of deteriorating quality of care during labour and vaginal birth, fostering the feeling that CS was the safest option. Health professionals' preference for CS was influenced by financial drivers and malpractice fears. This review has some limitations, including high heterogeneity (despite subgroup and sensitivity analysis) in the quantitative analysis, and the potential for over-reporting of women's preferences for CS in the qualitative synthesis (due to some included studies only including women who requested CS).
Conclusions: Despite a minority of women expressing a preference for CS, individual, health system, and socio-cultural factors converge, contributing to a high CS rate in mainland China, Hong Kong, and Taiwan. In order to reduce unnecessary CSs, interventions need to address all these non-clinical factors and concerns.
Systematic review registry: Prospero CRD42016036596.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
Cesarean section in China, Taiwan, and Hong Kong-A safe choice for women and clinicians?PLoS Med. 2018 Oct 16;15(10):e1002676. doi: 10.1371/journal.pmed.1002676. eCollection 2018 Oct. PLoS Med. 2018. PMID: 30325917 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
