

Association of Gleason Grade With Androgen Deprivation Therapy Duration and Survival Outcomes: A Systematic Review and Patient-Level Meta-analysis
- PMID: 30326032
- PMCID: PMC6440243
- DOI: 10.1001/jamaoncol.2018.3732
Association of Gleason Grade With Androgen Deprivation Therapy Duration and Survival Outcomes: A Systematic Review and Patient-Level Meta-analysis
Abstract
Importance: Androgen deprivation therapy (ADT) improves survival outcomes in patients with high-risk prostate cancer (PCa) treated with radiotherapy (RT). Whether this benefit differs between patients with Gleason grade group (GG) 4 (formerly Gleason score 8) and GG 5 (formerly Gleason score 9-10) disease remains unknown.
Objective: To determine whether the effectiveness of ADT duration varies between patients with GG 4 vs GG 5 PCa.
Design, setting, and participants: Traditional and network individual patient data meta-analyses of 992 patients (593 GG 4 and 399 GG 5) who were enrolled in 6 randomized clinical trials were carried out.
Main outcomes and measures: Multivariable Cox proportional hazard models were used to obtain hazard ratio (HR) estimates of ADT duration effects on overall survival (OS) and distant metastasis-free survival (DMFS). Cause-specific competing risk models were used to estimate HRs for cancer-specific survival (CSS). The interaction of ADT with GS was incorporated into the multivariable models. Traditional and network meta-analysis frameworks were used to compare outcomes of patients treated with RT alone, short-term ADT (STADT), long-term ADT (LTADT), and lifelong ADT.
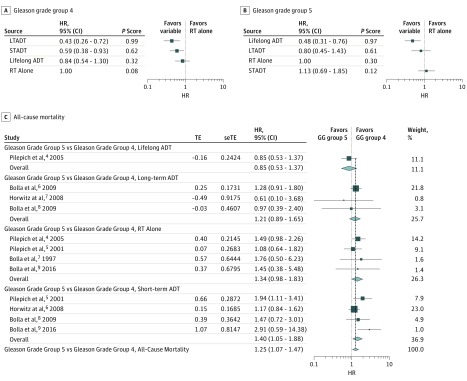
Results: Five hundred ninety-three male patients (mean age, 70 years; range, 43-88 years) with GG 4 and 399 with GG 5 were identified. Median follow-up was 6.4 years. Among GG 4 patients, LTADT and STADT improved OS over RT alone (HR, 0.43; 95% CI, 0.26-0.70 and HR, 0.59; 95% CI, 0.38-0.93, respectively; P = .03 for both), whereas lifelong ADT did not (HR, 0.84; 95% CI, 0.54-1.30; P = .44). Among GG 5 patients, lifelong ADT improved OS (HR, 0.48; 95% CI, 0.31-0.76; P = .04), whereas neither LTADT nor STADT did (HR, 0.80; 95% CI, 0.45-1.44 and HR, 1.13; 95% CI, 0.69-1.87; P = .45 and P = .64, respectively). Among all patients, and among those receiving STADT, GG 5 patients had inferior OS compared with GG 4 patients (HR, 1.25; 95% CI, 1.07-1.47 and HR, 1.40; 95% CI, 1.05-1.88, respectively; P = .02). There was no significant OS difference between GG 5 and GG 4 patients receiving LTADT or lifelong ADT (HR, 1.21; 95% CI, 0.89-1.65 and HR, 0.85; 95% CI, 0.53-1.37; P = .23 and P = .52, respectively).
Conclusions and relevance: These data suggest that prolonged durations of ADT improve survival outcomes in both GG 4 disease and GG 5 disease, albeit with different optimal durations. Strategies to maintain the efficacy of ADT while minimizing its duration (potentially with enhanced potency agents) should be investigated.
Conflict of interest statement
Figures
Comment in
-
Effects of androgen deprivation therapy duration and Gleason grade on survival outcomes of high risk prostate cancer.Transl Cancer Res. 2019 Jun;8(3):715-718. doi: 10.21037/tcr.2019.04.05. Transl Cancer Res. 2019. PMID: 35116806 Free PMC article. No abstract available.
-
Androgen deprivation therapy and Gleason grade: unravelling implications on survival.Transl Cancer Res. 2019 Jun;8(3):729-731. doi: 10.21037/tcr.2019.04.12. Transl Cancer Res. 2019. PMID: 35116810 Free PMC article. No abstract available.
References
-
- Pilepich MV, Winter K, John MJ, et al. Phase III radiation therapy oncology group (RTOG) trial 86-10 of androgen deprivation adjuvant to definitive radiotherapy in locally advanced carcinoma of the prostate. Int J Radiat Oncol Biol Phys. 2001;50(5):1243-1252. doi: 10.1016/S0360-3016(01)01579-6 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
