

Association of Genetically Enhanced Lipoprotein Lipase-Mediated Lipolysis and Low-Density Lipoprotein Cholesterol-Lowering Alleles With Risk of Coronary Disease and Type 2 Diabetes
- PMID: 30326043
- PMCID: PMC6217943
- DOI: 10.1001/jamacardio.2018.2866
Association of Genetically Enhanced Lipoprotein Lipase-Mediated Lipolysis and Low-Density Lipoprotein Cholesterol-Lowering Alleles With Risk of Coronary Disease and Type 2 Diabetes
Abstract
Importance: Pharmacological enhancers of lipoprotein lipase (LPL) are in preclinical or early clinical development for cardiovascular prevention. Studying whether these agents will reduce cardiovascular events or diabetes risk when added to existing lipid-lowering drugs would require large outcome trials. Human genetics studies can help prioritize or deprioritize these resource-demanding endeavors.
Objective: To investigate the independent and combined associations of genetically determined differences in LPL-mediated lipolysis and low-density lipoprotein cholesterol (LDL-C) metabolism with risk of coronary disease and diabetes.
Design, setting, and participants: In this genetic association study, individual-level genetic data from 392 220 participants from 2 population-based cohort studies and 1 case-cohort study conducted in Europe were included. Data were collected from January 1991 to July 2018, and data were analyzed from July 2014 to July 2018.
Exposures: Six conditionally independent triglyceride-lowering alleles in LPL, the p.Glu40Lys variant in ANGPTL4, rare loss-of-function variants in ANGPTL3, and LDL-C-lowering polymorphisms at 58 independent genomic regions, including HMGCR, NPC1L1, and PCSK9.
Main outcomes and measures: Odds ratio for coronary artery disease and type 2 diabetes.
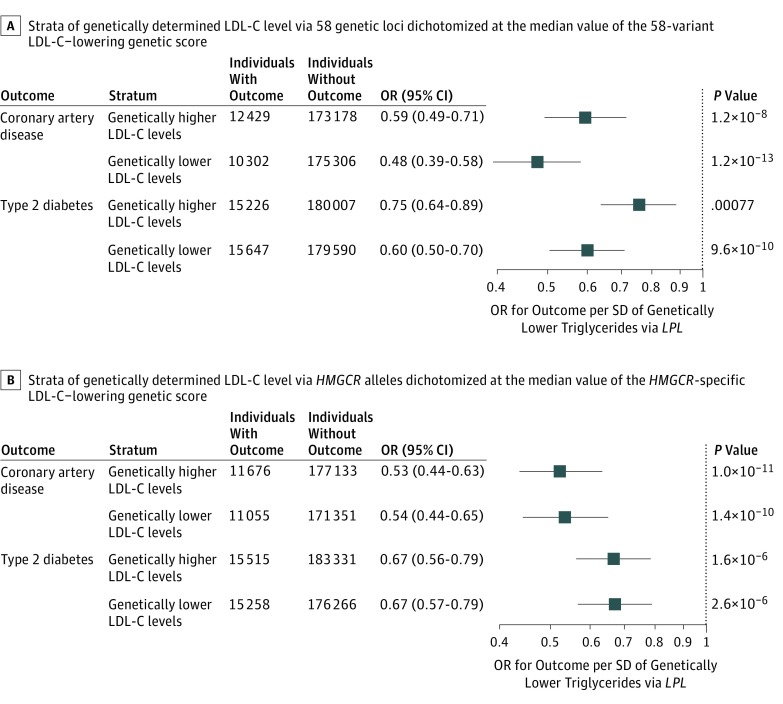
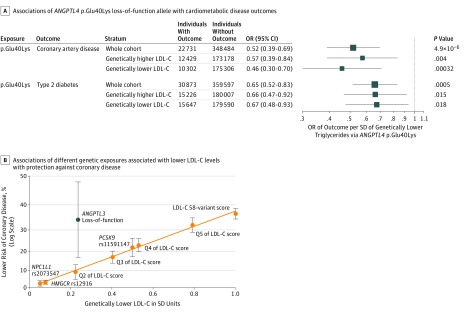
Results: Of the 392 220 participants included, 211 915 (54.0%) were female, and the mean (SD) age was 57 (8) years. Triglyceride-lowering alleles in LPL were associated with protection from coronary disease (approximately 40% lower odds per SD of genetically lower triglycerides) and type 2 diabetes (approximately 30% lower odds) in people above or below the median of the population distribution of LDL-C-lowering alleles at 58 independent genomic regions, HMGCR, NPC1L1, or PCSK9. Associations with lower risk were consistent in quintiles of the distribution of LDL-C-lowering alleles and 2 × 2 factorial genetic analyses. The 40Lys variant in ANGPTL4 was associated with protection from coronary disease and type 2 diabetes in groups with genetically higher or lower LDL-C. For a genetic difference of 0.23 SDs in LDL-C, ANGPTL3 loss-of-function variants, which also have beneficial associations with LPL lipolysis, were associated with greater protection against coronary disease than other LDL-C-lowering genetic mechanisms (ANGPTL3 loss-of-function variants: odds ratio, 0.66; 95% CI, 0.52-0.83; 58 LDL-C-lowering variants: odds ratio, 0.90; 95% CI, 0.89-0.91; P for heterogeneity = .009).
Conclusions and relevance: Triglyceride-lowering alleles in the LPL pathway are associated with lower risk of coronary disease and type 2 diabetes independently of LDL-C-lowering genetic mechanisms. These findings provide human genetics evidence to support the development of agents that enhance LPL-mediated lipolysis for further clinical benefit in addition to LDL-C-lowering therapy.
Conflict of interest statement
Figures


Comment in
-
Opportunities and Challenges in Mendelian Randomization Studies to Guide Trial Design.JAMA Cardiol. 2018 Oct 1;3(10):967. doi: 10.1001/jamacardio.2018.2863. JAMA Cardiol. 2018. PMID: 30326490 No abstract available.
Similar articles
-
Association Between Low-Density Lipoprotein Cholesterol-Lowering Genetic Variants and Risk of Type 2 Diabetes: A Meta-analysis.JAMA. 2016 Oct 4;316(13):1383-1391. doi: 10.1001/jama.2016.14568. JAMA. 2016. PMID: 27701660 Free PMC article.
-
Evaluating the Cardiometabolic Efficacy and Safety of Lipoprotein Lipase Pathway Targets in Combination With Approved Lipid-Lowering Targets: A Drug Target Mendelian Randomization Study.Circ Genom Precis Med. 2025 Apr;18(2):e004933. doi: 10.1161/CIRCGEN.124.004933. Epub 2025 Mar 7. Circ Genom Precis Med. 2025. PMID: 40052268 Free PMC article.
-
Association of Triglyceride-Lowering LPL Variants and LDL-C-Lowering LDLR Variants With Risk of Coronary Heart Disease.JAMA. 2019 Jan 29;321(4):364-373. doi: 10.1001/jama.2018.20045. JAMA. 2019. PMID: 30694319 Free PMC article.
-
Regulation of lipoprotein lipase-mediated lipolysis of triglycerides.Curr Opin Lipidol. 2020 Jun;31(3):154-160. doi: 10.1097/MOL.0000000000000676. Curr Opin Lipidol. 2020. PMID: 32332431 Free PMC article. Review.
-
Genetic Association of Lipids and Lipid Drug Targets With Abdominal Aortic Aneurysm: A Meta-analysis.JAMA Cardiol. 2018 Jan 1;3(1):26-33. doi: 10.1001/jamacardio.2017.4293. JAMA Cardiol. 2018. PMID: 29188294 Free PMC article. Review.
Cited by
-
Role of angiopoietin-like protein 3 in sugar-induced dyslipidemia in rhesus macaques: suppression by fish oil or RNAi.J Lipid Res. 2020 Mar;61(3):376-386. doi: 10.1194/jlr.RA119000423. Epub 2020 Jan 9. J Lipid Res. 2020. PMID: 31919051 Free PMC article.
-
Dual role of ANGPTL4 in inflammation.Inflamm Res. 2023 Jun;72(6):1303-1313. doi: 10.1007/s00011-023-01753-9. Epub 2023 Jun 10. Inflamm Res. 2023. PMID: 37300585 Free PMC article. Review.
-
Metabolic profiling of angiopoietin-like protein 3 and 4 inhibition: a drug-target Mendelian randomization analysis.Eur Heart J. 2021 Mar 21;42(12):1160-1169. doi: 10.1093/eurheartj/ehaa972. Eur Heart J. 2021. PMID: 33351885 Free PMC article.
-
Emerging Targets for Cardiovascular Disease Prevention in Diabetes.Trends Mol Med. 2020 Aug;26(8):744-757. doi: 10.1016/j.molmed.2020.03.011. Epub 2020 May 15. Trends Mol Med. 2020. PMID: 32423639 Free PMC article. Review.
-
Regulation of plasma triglyceride partitioning by adipose-derived ANGPTL4 in mice.Sci Rep. 2021 Apr 12;11(1):7873. doi: 10.1038/s41598-021-87020-5. Sci Rep. 2021. PMID: 33846453 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
- 098381/WT_/Wellcome Trust/United Kingdom
- 115372/DH_/Department of Health/United Kingdom
- RG/13/13/30194/BHF_/British Heart Foundation/United Kingdom
- 095515/Z/11/Z/WT_/Wellcome Trust/United Kingdom
- MR/N003284/1/MRC_/Medical Research Council/United Kingdom
- 204623/WT_/Wellcome Trust/United Kingdom
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- 14136/CRUK_/Cancer Research UK/United Kingdom
- 100574/Z/12/Z/WT_/Wellcome Trust/United Kingdom
- 204623/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MC_PC_13048/MRC_/Medical Research Council/United Kingdom
- G1000143/MRC_/Medical Research Council/United Kingdom
- MC_UU_12012/5/MRC_/Medical Research Council/United Kingdom
- MC_UU_12015/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00002/7/MRC_/Medical Research Council/United Kingdom
- MC_PC_13046/MRC_/Medical Research Council/United Kingdom
- MC_UU_12015/2/MRC_/Medical Research Council/United Kingdom
- G0401527/MRC_/Medical Research Council/United Kingdom
- MR/L00002/1/MRC_/Medical Research Council/United Kingdom
- 090532/WT_/Wellcome Trust/United Kingdom
- 107064/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
