

Outcomes of Open vs Endoscopic Skull Base Surgery in Patients 70 Years or Older
- PMID: 30326054
- PMCID: PMC6233820
- DOI: 10.1001/jamaoto.2018.1948
Outcomes of Open vs Endoscopic Skull Base Surgery in Patients 70 Years or Older
Abstract
Importance: The use of skull base surgery in patients 70 years or older is increasing, but its safety in this age group has not been evaluated to date.
Objectives: To describe outcomes in a cohort of patients 70 years or older undergoing skull base surgery and to evaluate whether age, type of disease process, and approach (endoscopic vs traditional open surgery) are associated with increased intraoperative and postoperative complications in this population.
Design, setting, and participants: This retrospective cohort study analyzed a population-based sample of 219 patients 70 years or older from a database of 1720 patients who underwent skull base surgery at University of North Carolina Hospitals, Chapel Hill, a tertiary referral center, between October 2007 and June 2017. Data were collected from June 2016 to July 2017 and analyzed in July 2017 and August 2017.
Exposure: Skull base surgery.
Main outcomes and measures: Data collected included demographic characteristics, surgical approach, and disease process. Intraoperative findings and postoperative complications were analyzed by age, surgical approach, and malignancy status.
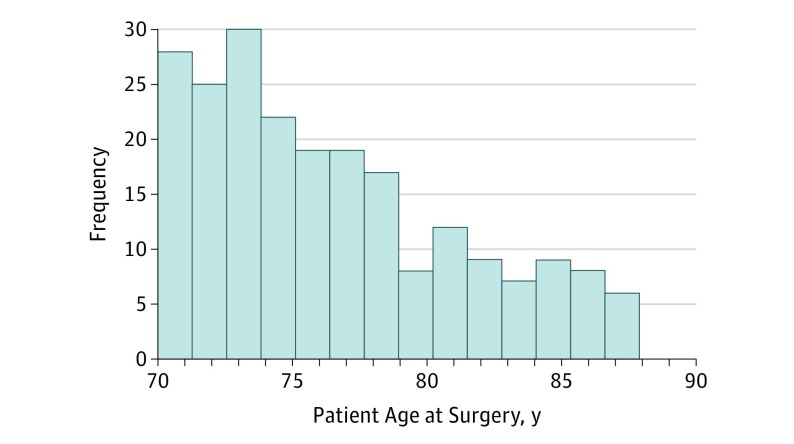
Results: Of the 219 patients, 166 were aged 70.0 to 79.9 years and 53 patients were older than 80 years (mean [SD] age, 76.4 [4.7] years); 120 (54.8%) were men and 160 (73.7%) were white. There were 161 (73.5%) endoscopic and 58 (26.5%) open operations. The most common pathologic processes among the 219 patients were nonsellar malignant (81 [37.0%]), nonsellar benign (53 [24.2%]), and pituitary (49 [22.4%]) tumors. The most common intraoperative and postoperative complications were intraoperative major bleeding (5 of 219 patients [2.3%]) and postoperative bleeding (9 [4.1%]). Thirty-day mortality was zero. There was no clinically meaningful difference in complications between patients aged 70.0 to 79.9 years vs those older than 80 years, endoscopic vs open surgery, or benign vs malignant neoplasms. Specifically, between the endoscopic and open surgery groups, there was no difference in intraoperative major bleeding (3.9%; 95% CI, -0.7% to 12.9%), postoperative cerebrospinal fluid leak (-0.6%; 95% CI, -3.4% to 5.6%), or postoperative bleeding (1.5%; 95% CI, -3.9% to 10.6%).
Conclusions and relevance: Skull base surgery is a safe option in persons 70 years or older, with similar outcomes across age ranges, surgical approaches, and disease processes.
Conflict of interest statement
Figures
Similar articles
-
Outcomes of Endoscopic Versus Open Skull Base Surgery in Pediatric Patients.Laryngoscope. 2021 May;131(5):996-1001. doi: 10.1002/lary.29127. Epub 2020 Nov 2. Laryngoscope. 2021. PMID: 33135787
-
Risk factors associated with postoperative cerebrospinal fluid leak after endoscopic endonasal skull base surgery.J Neurosurg. 2018 Apr;128(4):1066-1071. doi: 10.3171/2016.12.JNS1694. Epub 2017 Jun 9. J Neurosurg. 2018. PMID: 28598276
-
Outcomes and complications of endoscopic approaches for malignancies of the paranasal sinuses and anterior skull base.Ann Otol Rhinol Laryngol. 2013 Jan;122(1):54-9. doi: 10.1177/000348941312200110. Ann Otol Rhinol Laryngol. 2013. PMID: 23472317
-
Endoscopic endonasal versus open transcranial resection of anterior midline skull base meningiomas.World Neurosurg. 2012 May-Jun;77(5-6):713-24. doi: 10.1016/j.wneu.2011.08.025. Epub 2011 Nov 7. World Neurosurg. 2012. PMID: 22120296 Review.
-
The awake endoscope-guided sealant technique with fibrin glue in the treatment of postoperative cerebrospinal fluid leak after extended transsphenoidal surgery: technical note.World Neurosurg. 2014 Sep-Oct;82(3-4):e479-85. doi: 10.1016/j.wneu.2013.01.017. Epub 2013 Jan 8. World Neurosurg. 2014. PMID: 23313259 Review.
Cited by
-
Impact of age on postsurgical outcomes of nonfunctioning pituitary adenomas.Endocrine. 2021 Jun;72(3):915-922. doi: 10.1007/s12020-020-02554-4. Epub 2020 Nov 26. Endocrine. 2021. PMID: 33242176
-
Complications After Open Skull Base Surgery for Brain Tumors: A 26-Year Experience.Cureus. 2023 Dec 11;15(12):e50312. doi: 10.7759/cureus.50312. eCollection 2023 Dec. Cureus. 2023. PMID: 38205474 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
