

Use and Cost of Actinic Keratosis Destruction in the Medicare Part B Fee-for-Service Population, 2007 to 2015
- PMID: 30326488
- PMCID: PMC6248125
- DOI: 10.1001/jamadermatol.2018.3086
Use and Cost of Actinic Keratosis Destruction in the Medicare Part B Fee-for-Service Population, 2007 to 2015
Abstract
Importance: Actinic keratosis is prevalent and has the potential to progress to keratinocyte carcinoma. Changes in the use and costs of actinic keratosis treatment are not well understood in the aging population.
Objective: To evaluate trends in the use and costs of actinic keratosis destruction in Medicare patients.
Design, setting, and participants: A billing claims analysis was performed of the Medicare Part B Physician/Supplier Procedure Summary Master Files and National Summary Data of premalignant skin lesion destructions performed from 2007 to 2015 among Medicare Part B fee-for-service beneficiaries.
Main outcomes and measures: Mean number of actinic keratosis lesions destroyed and associated treatment payments in 2015 US dollars estimated per 1000 Medicare Part B fee-for-service beneficiaries. Data analysis was performed from November 2017 to July 2018.
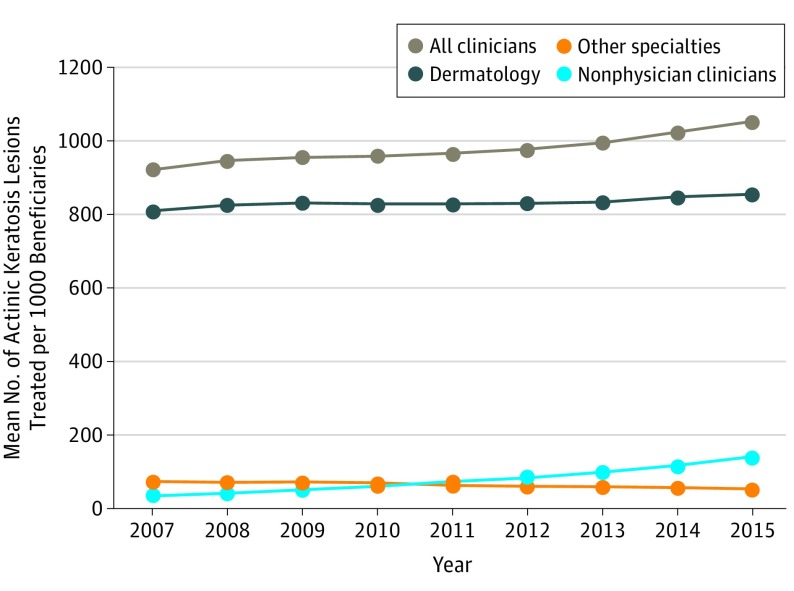
Results: More than 35.6 million actinic keratosis lesions were treated in 2015, increasing from 29.7 million in 2007. Treated actinic keratosis lesions per 1000 beneficiaries increased from 917 in 2007 to 1051 in 2015, while mean inflation-adjusted payments per 1000 patients decreased from $11 749 to $10 942 owing to reimbursement cuts. The proportion of actinic keratosis lesions treated by independently billing nurse practitioners and physician assistants increased from 4.0% in 2007 to 13.5% in 2015.
Conclusions and relevance: This study's findings suggest that actinic keratosis imposes continuously increasing levels of treatment burden in the Medicare fee-for-service population. Reimbursement decreases have been used to control rising costs of actinic keratosis treatment. Critical research may be warranted to optimize access to actinic keratosis treatment and value for prevention of keratinocyte carcinoma.
Conflict of interest statement
Figures

Comment in
-
Translating Administrative Health Care Data to Treatment Decisions in Dermatology: The Blind Men and the Elephant.JAMA Dermatol. 2018 Nov 1;154(11):1256-1257. doi: 10.1001/jamadermatol.2018.3063. JAMA Dermatol. 2018. PMID: 30326491 No abstract available.
References
-
- Landis ET, Davis SA, Taheri A, Feldman SR. Top dermatologic diagnoses by age. Dermatol Online J. 2014;20(4):22368. - PubMed
-
- Tennvall GR, Norlin JM, Malmberg I, Erlendsson AM, Hædersdal M. Health related quality of life in patients with actinic keratosis—an observational study of patients treated in dermatology specialist care in Denmark. Health Qual Life Outcomes. 2015;13:111. doi: 10.1186/s12955-015-0295-4 - DOI - PMC - PubMed
-
- Philipp-Dormston WG, Müller K, Novak B, et al. ; NMSC-QoL Study Group . Patient-reported health outcomes in patients with non-melanoma skin cancer and actinic keratosis: results from a large-scale observational study analysing effects of diagnoses and disease progression. J Eur Acad Dermatol Venereol. 2018;32(7):1138-1146. doi: 10.1111/jdv.14703 - DOI - PMC - PubMed
