

High-flow nasal cannula in adults with acute respiratory failure and after extubation: a systematic review and meta-analysis
- PMID: 30326893
- PMCID: PMC6192218
- DOI: 10.1186/s12931-018-0908-7
High-flow nasal cannula in adults with acute respiratory failure and after extubation: a systematic review and meta-analysis
Abstract
Background: High-flow nasal cannula (HFNC) can be used as an initial support strategy for patients with acute respiratory failure (ARF) and after extubation. However, no clear evidence exists to support or oppose HFNC use in clinical practice. We summarized the effects of HFNC, compared to conventional oxygen therapy (COT) and noninvasive ventilation (NIV), on important outcomes including treatment failure and intubation/reintubation rates in adult patients with ARF and after extubation.
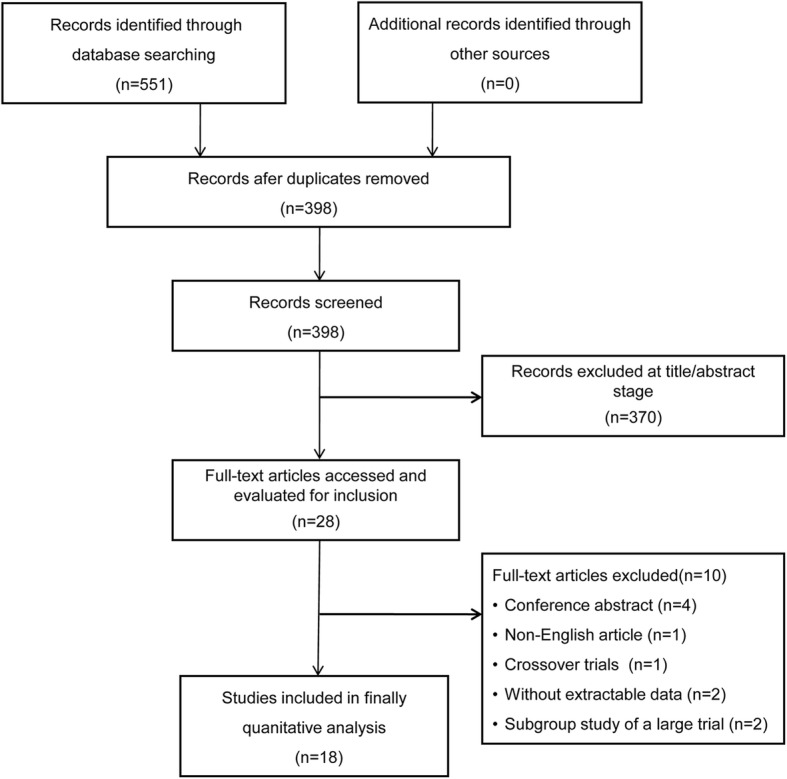
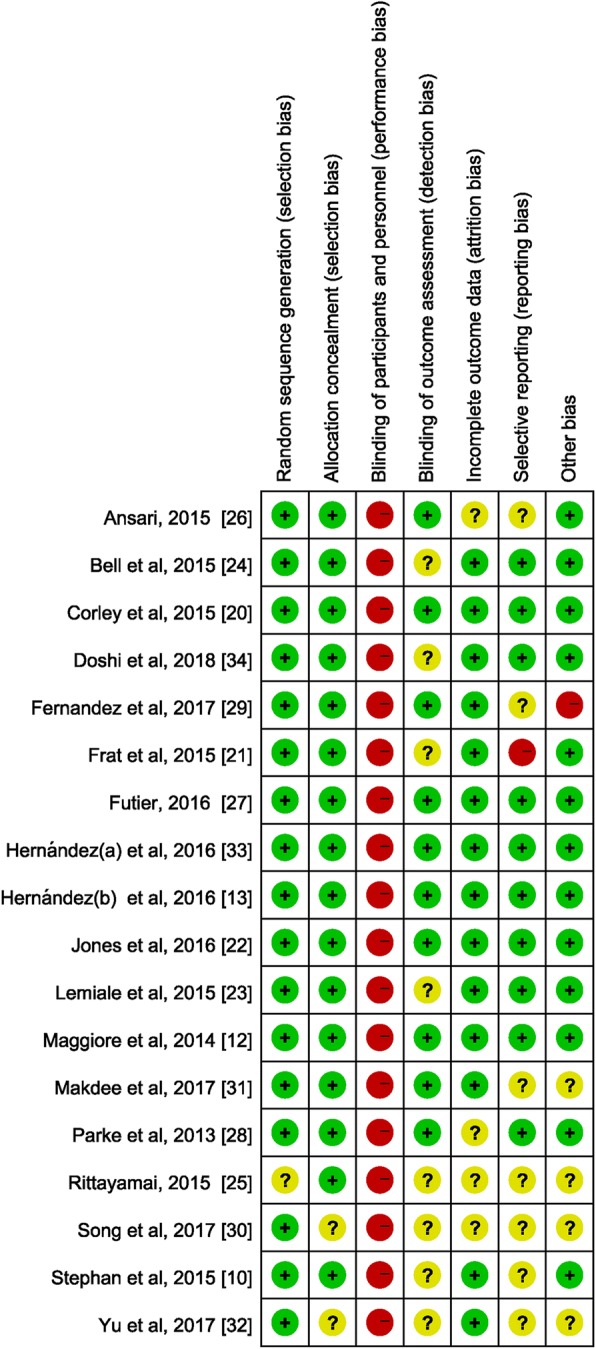
Methods: We searched 4 electronic databases (Pubmed, EMBASE, Scopus, and Web of Science) to identify randomized controlled trials (RCTs) comparing the effects of HFNC with either COT or NIV on rates of 1) treatment failure and 2) intubation/reintubation in adult critically ill patients.
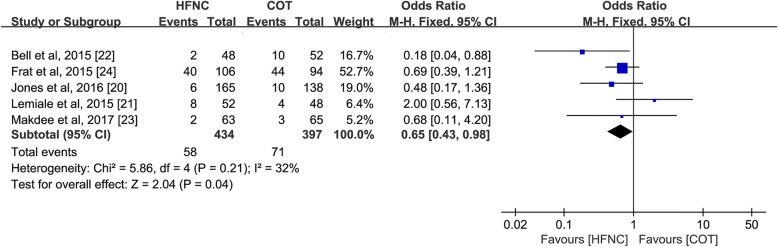
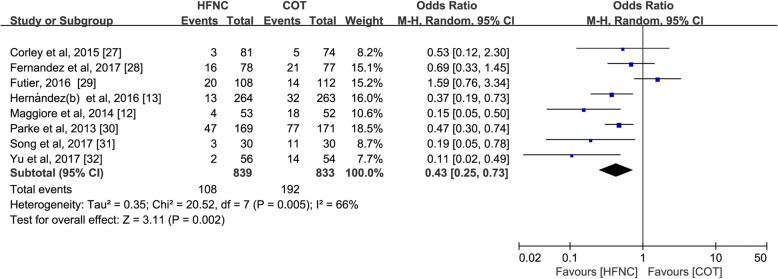
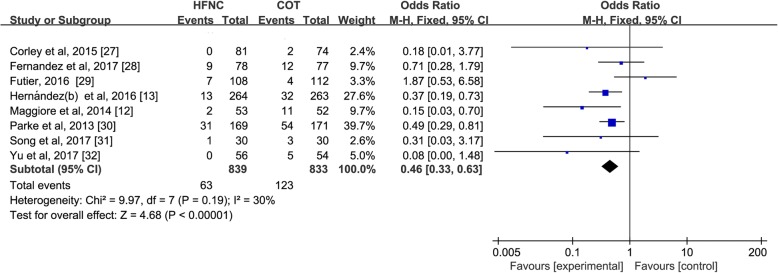
Results: We identified 18 RCTs (n = 4251 patients) in pooled analyses. As a primary mode of support, HFNC treatment reduced the risk of treatment failure [Odds Ratio (OR) 0.65; 95% confidence interval (CI) 0.43-0.98; p = 0.04; I2 = 32%] but had no effect on preventing intubation (OR, 0.74; 95%CI 0.45-1.21; p = 0.23; I2 = 0%) compared to COT. When used after extubation, HFNC (vs. COT) treatment significantly decreased reintubation rate (OR 0.46; 95%CI 0.33-0.63; p < 0.00001; I2 = 30%) and extubation failure (OR 0.43; 95%CI 0.25-0.73; p = 0.002; I2 = 66%). Compared to NIV, HFNC significantly reduced intubation rate (OR 0.57; 95%CI 0.36-0.92; p = 0.02; I2 = 0%) when used as initial support, but did no favorably impact clinical outcomes post extubation in few trials.
Conclusions: HFNC was superior to COT in reducing treatment failure when used as a primary support strategy and in reducing rates of extubation failure and reintubation when used after extubation. In few trials, HFNC reduced intubation rate compared to NIV when used as initial support but demonstrated no beneficial effects after extubation.
Keywords: Conventional oxygen therapy; Extubation; Noninvasive ventilation.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- O'Driscoll BR, Howard LS, Davison AG. BTS guideline for emergency oxygen use in adult patients. Thorax. 2008;63(Suppl 6):vi1–v68. - PubMed
-
- Roca O, Hernandez G, Diaz-Lobato S, Carratala JM, Gutierrez RM, Masclans JR, et al. Current evidence for the effectiveness of heated and humidified high flow nasal cannula supportive therapy in adult patients with respiratory failure. Crit Care. 2016;20(1):109. doi: 10.1186/s13054-016-1263-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
