

Gender differences in tuberculosis treatment outcomes: a post hoc analysis of the REMoxTB study
- PMID: 30326959
- PMCID: PMC6192317
- DOI: 10.1186/s12916-018-1169-5
Gender differences in tuberculosis treatment outcomes: a post hoc analysis of the REMoxTB study
Abstract
Background: In the REMoxTB study of 4-month treatment-shortening regimens containing moxifloxacin compared to the standard 6-month regimen for tuberculosis, the proportion of unfavourable outcomes for women was similar in all study arms, but men had more frequent unfavourable outcomes (bacteriologically or clinically defined failure or relapse within 18 months after randomisation) on the shortened moxifloxacin-containing regimens. The reason for this gender disparity in treatment outcome is poorly understood.
Methods: The gender differences in baseline variables were calculated, as was time to smear and culture conversion and Kaplan-Meier plots were constructed. In post hoc exploratory analyses, multivariable logistic regression modelling and an observed case analysis were used to explore factors associated with both gender and unfavourable treatment outcome.
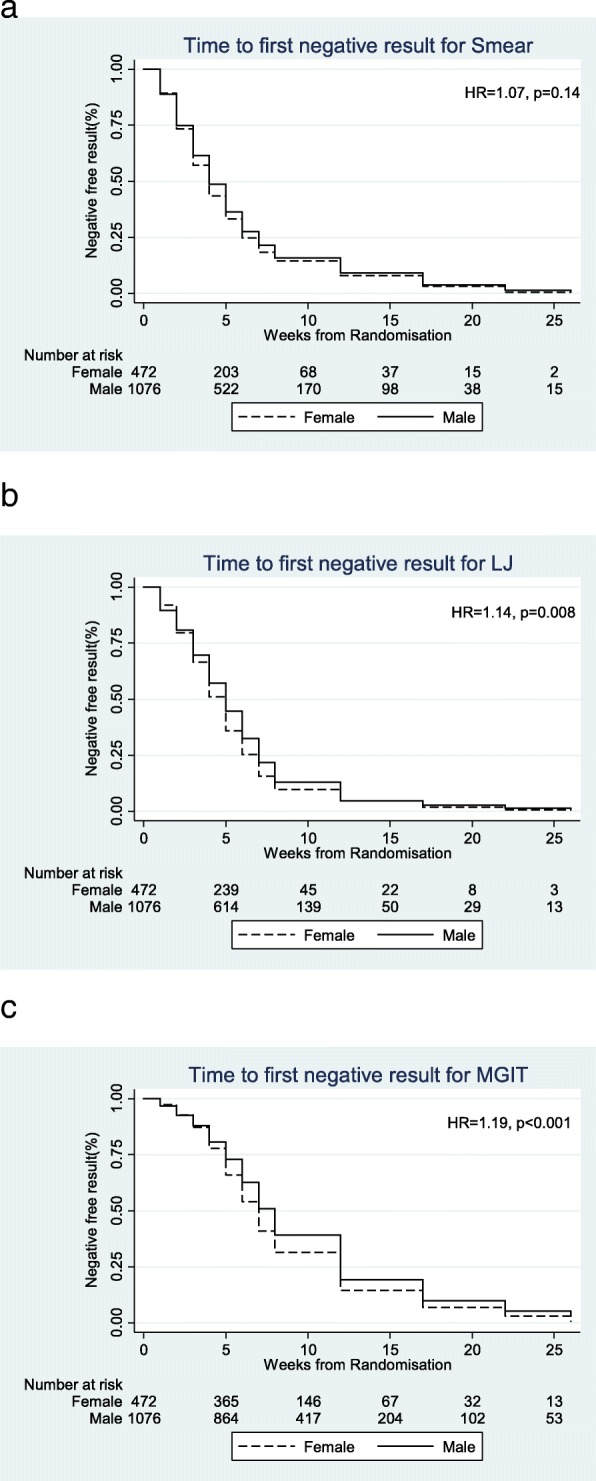
Results: The per-protocol population included 472/1548 (30%) women. Women were younger and had lower rates of cavitation, smoking and weight (all p < 0.05) and higher prevalence of HIV (10% vs 6%, p = 0.001). They received higher doses (mg/kg) than men of rifampicin, isoniazid, pyrazinamide and moxifloxacin (p ≤ 0.005). There was no difference in baseline smear grading or mycobacterial growth indicator tube (MGIT) time to positivity. Women converted to negative cultures more quickly than men on Lowenstein-Jensen (HR 1.14, p = 0.008) and MGIT media (HR 1.19, p < 0.001). In men, the presence of cavitation, positive HIV status, higher age, lower BMI and 'ever smoked' were independently associated with unfavourable treatment outcome. In women, only 'ever smoked' was independently associated with unfavourable treatment outcome. Only for cavitation was there a gender difference in treatment outcomes by regimen; their outcome in the 4-month arms was significantly poorer compared to the 6-month treatment arm (p < 0.001). Women, with or without cavities, and men without cavities had a similar outcome on all treatment arms (p = 0.218, 0.224 and 0.689 respectively). For all other covariate subgroups, there were no differences in treatment effects for men or women.
Conclusions: Gender differences in TB treatment responses for the shorter regimens in the REMoxTB study may be explained by poor outcomes in men with cavitation on the moxifloxacin-containing regimens. We observed that women with cavities, or without, on the 4-month moxifloxacin regimens had similar outcomes to all patients on the standard 6-month treatment. The biological reasons for this difference are poorly understood and require further exploration.
Keywords: Cavitation; Clinical trials; Gender; REMoxTB; Treatment outcome; Tuberculosis.
Conflict of interest statement
Authors’ information
MM—UCL Clinician and Research Associate; GW—Statistician, MRC Clinical Trials Unit at UCL; SM—Clinician and Research Associate, UCL; CL—Clinician and Principal Investigator, Madibeng Centre for Research, South Africa; AB—Post-doctoral Scientist, UCL; RH—Senior Research Associate, UCL; TDM—Professor of Clinical Microbiology, UCL, and Director, UCL Centre for Clinical Microbiology; AJN—Senior scientist at MRC Clinical Trials Unit at UCL; SKM—Professor of Clinical Trials, MRC Clinical Trials Unit at UCL; CM—Senior VP Research and Development, TB Alliance; MS—President and CEO, TB Alliance; AC—Senior Statistician, MRC Clinical Trials Unit at UCL; SHG—Sir James Black Professor of Medicine, University of St Andrews.
Ethics approval and consent to participate
The UCL ethics committee and the ethics committees of all study sites and organisations approved the REMoxTB study; these are provided in the Additional file 2. Patients gave their informed consent for the REMoxTB study and for their specimens and data to be used for the purposes of this study [10].
Consent for publication
All authors have given their consent to publication and have agreed to the authorship and order of authorship for this manuscript.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO . Global tuberculosis report. 2015.
-
- WHO . Tuberculosis in women. 2014.
-
- Weiss MG, Sommerfeld J, Uplekar MW. Social and cultural dimensions of gender and tuberculosis. Int J Tuberc Lung Dis. 2008;12(7):829–830. - PubMed
-
- Horton Katherine C., MacPherson Peter, Houben Rein M. G. J., White Richard G., Corbett Elizabeth L. Sex Differences in Tuberculosis Burden and Notifications in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis. PLOS Medicine. 2016;13(9):e1002119. doi: 10.1371/journal.pmed.1002119. - DOI - PMC - PubMed
-
- Gosoniu GD, Ganapathy S, Kemp J, Auer C, Somma D, Karim F, Weiss MG. Gender and socio-cultural determinants of delay to diagnosis of TB in Bangladesh, India and Malawi. Int J Tuberc Lung Dis. 2008;12(7):848–855. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
