

Fasting and cancer: molecular mechanisms and clinical application
- PMID: 30327499
- PMCID: PMC6938162
- DOI: 10.1038/s41568-018-0061-0
Fasting and cancer: molecular mechanisms and clinical application
Abstract
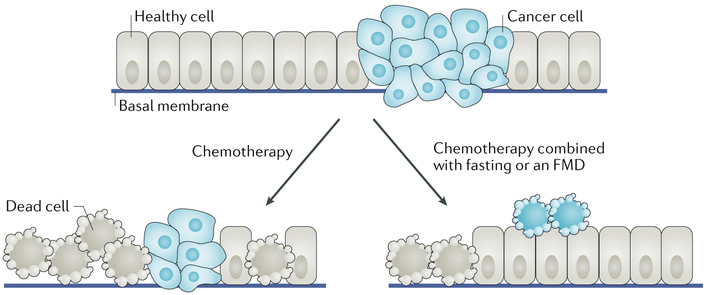
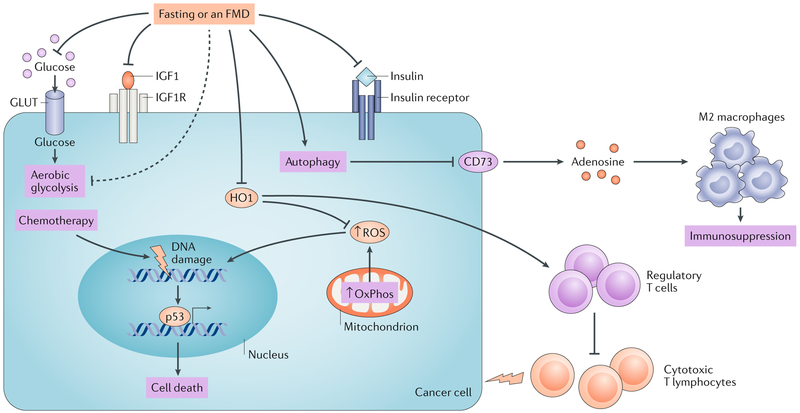
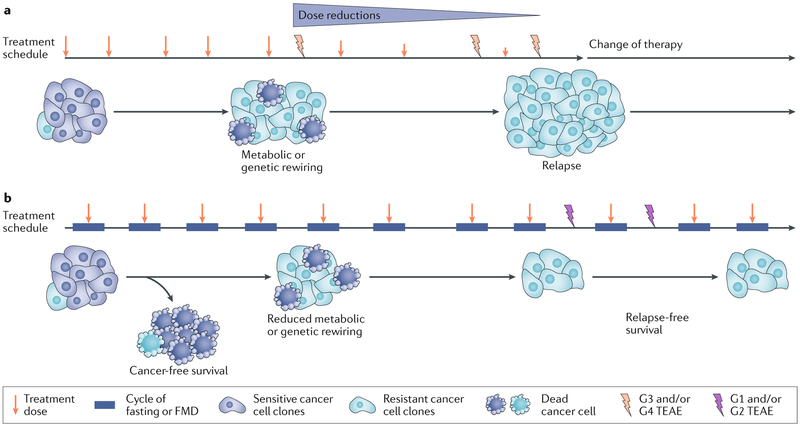
The vulnerability of cancer cells to nutrient deprivation and their dependency on specific metabolites are emerging hallmarks of cancer. Fasting or fasting-mimicking diets (FMDs) lead to wide alterations in growth factors and in metabolite levels, generating environments that can reduce the capability of cancer cells to adapt and survive and thus improving the effects of cancer therapies. In addition, fasting or FMDs increase resistance to chemotherapy in normal but not cancer cells and promote regeneration in normal tissues, which could help prevent detrimental and potentially life-threatening side effects of treatments. While fasting is hardly tolerated by patients, both animal and clinical studies show that cycles of low-calorie FMDs are feasible and overall safe. Several clinical trials evaluating the effect of fasting or FMDs on treatment-emergent adverse events and on efficacy outcomes are ongoing. We propose that the combination of FMDs with chemotherapy, immunotherapy or other treatments represents a potentially promising strategy to increase treatment efficacy, prevent resistance acquisition and reduce side effects.
Conflict of interest statement
Competing interests
A.N. and I.C. are inventors on three patents of methods for treating cancer by fasting-mimicking diets that are currently under negotiation with L-Nutra Inc. V.D.L. is the founder of L-Nutra Inc.
Figures
Comment in
-
Reply to 'Fasting in oncology: a word of caution'.Nat Rev Cancer. 2019 Mar;19(3):178. doi: 10.1038/s41568-018-0100-x. Nat Rev Cancer. 2019. PMID: 30651605 No abstract available.
References
-
- Lanier AP, Bender TR, Blot WJ, Fraumeni JF Jr & Hurlburt WB Cancer incidence in Alaska natives. Int. J. Cancer 18, 409–412 (1976). - PubMed
-
- Henderson BE et al. Cancer incidence in the islands of the Pacific. Natl Cancer Inst. Monogr 69, 73–81 (1985). - PubMed
-
- Ziegler RG et al. Migration patterns and breast cancer risk in Asian-American women. J. Natl Cancer Inst 85, 1819–1827 (1993). - PubMed
-
- Le GM, Gomez SL, Clarke CA, Glaser SL & West DW Cancer incidence patterns among Vietnamese in the United States and Ha Noi, Vietnam. Int. J. Cancer 102, 412–417 (2002). - PubMed
-
- Hemminki K & Li X Cancer risks in second-generation immigrants to Sweden. Int. J. Cancer 99, 229–237 (2002). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
