

Acute multifocal retinitis: a retrospective review of 35 cases
- PMID: 30328571
- PMCID: PMC6192942
- DOI: 10.1186/s12348-018-0160-9
Acute multifocal retinitis: a retrospective review of 35 cases
Abstract
Background: Acute multifocal retinitis is a rare condition that has been considered to be often idiopathic. The purpose of this study was to analyze clinical features and causes of acute multifocal retinitis.
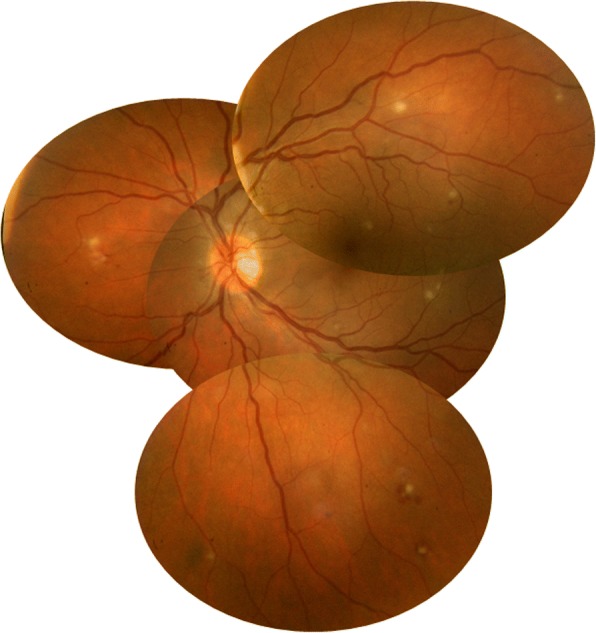
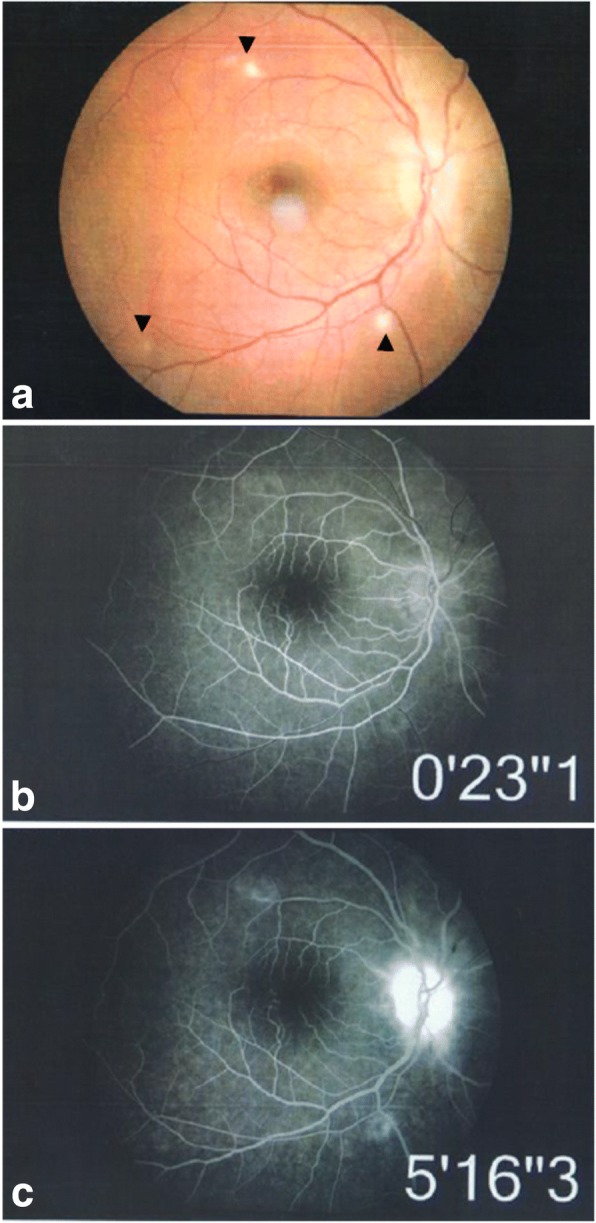
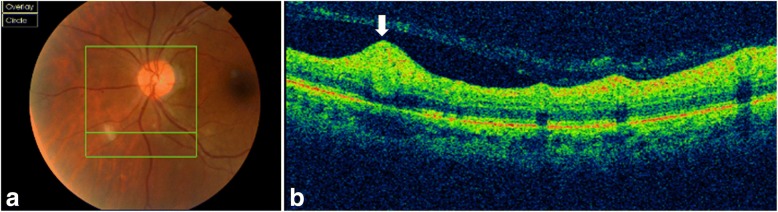
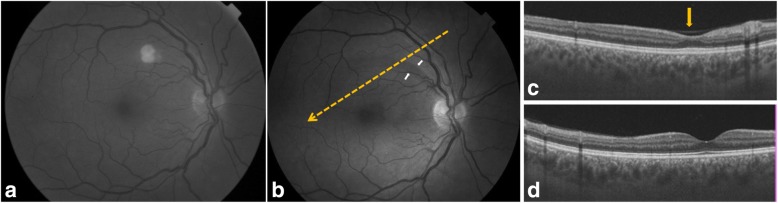
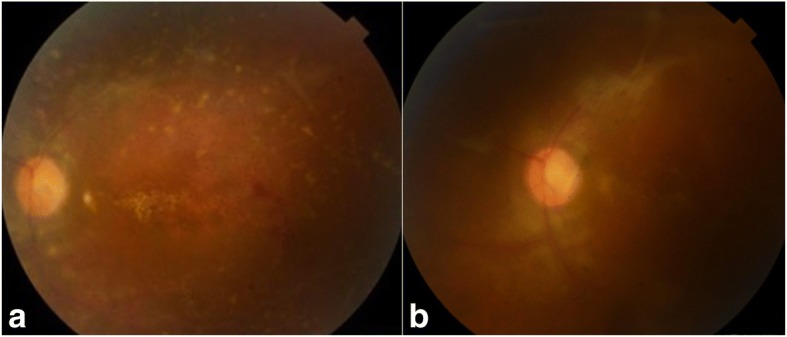
Results: This study is a retrospective review of the charts of 35 patients with acute multifocal retinitis. Patients with three or more retinal lesions in at least one eye, with at least one lesion of less than 500 μm in size were included. All patients had complete ophthalmological examination, fundus photography, and fluorescein angiography. Twelve patients (34.3%) had optical coherence tomography. An extensive work-up was performed including a detailed comprehensive medical history, examination by an internist and an infectious disease specialist, a chest X-ray, Mantoux test, and laboratory tests for syphilis, human immunodeficiency virus, Bartonella, and Rickettsia. Of the 35 patients, 25 (71.4%) had bilateral involvement and 10 (28.6%) had unilateral involvement (total number of eyes: 60). Mean best-corrected visual acuity (BCVA) was 20/25 (range, 20/1000-20/20). Retinal lesions ranged from 3 to more than 20 in number in at least 1 eye, and from 150 to 1500 μm in size. Associated findings included mild anterior chamber inflammation in 5 eyes (8.3%), mild vitritis in 46 eyes (76.7%), optic disc swelling in 9 eyes (15%), macular star in 4 eyes (6.7%), exudative retinal detachment in 6 eyes (10%), and branch retinal artery occlusion in 6 eyes (10%). Acute multifocal retinitis was found to be caused by Rickettsia conorii infection in 20 patients (57.1%), Rickettsia typhi infection in 4 patients (11.4%), cat-scratch disease in 8 patients (22.9%), and syphilis in 1 patient (2.9%). It was idiopathic in two patients (5.7%). Retinal lesions resolved without scarring in 3 to 12 weeks in all but three eyes (5%), in which residual retinal pigment epithelial changes were noted.
Conclusion: Rickettsial disease was the most common cause of acute multifocal retinitis. Other identified causes included cat-scratch disease and syphilis, and a very small subset of patients was diagnosed with idiopathic multifocal retinitis.
Keywords: Branch retinal artery occlusion; Cat-scratch disease; Posterior uveitis; Retinitis; Rickettsial disease.
Conflict of interest statement
Ethics approval and consent to participate
This work adheres to the guidelines and principles by the Declaration of Helsinki. It was approved by the ethics committee of our institution.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
