

Early versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
- PMID: 30328991
- PMCID: PMC6180467
- DOI: 10.5935/0103-507X.20180054
Early versus delayed initiation of renal replacement therapy for acute kidney injury: an updated systematic review, meta-analysis, meta-regression and trial sequential analysis of randomized controlled trials
Abstract
Objective: To evaluate whether early initiation of renal replacement therapy is associated with lower mortality in patients with acute kidney injury compared to delayed initiation.
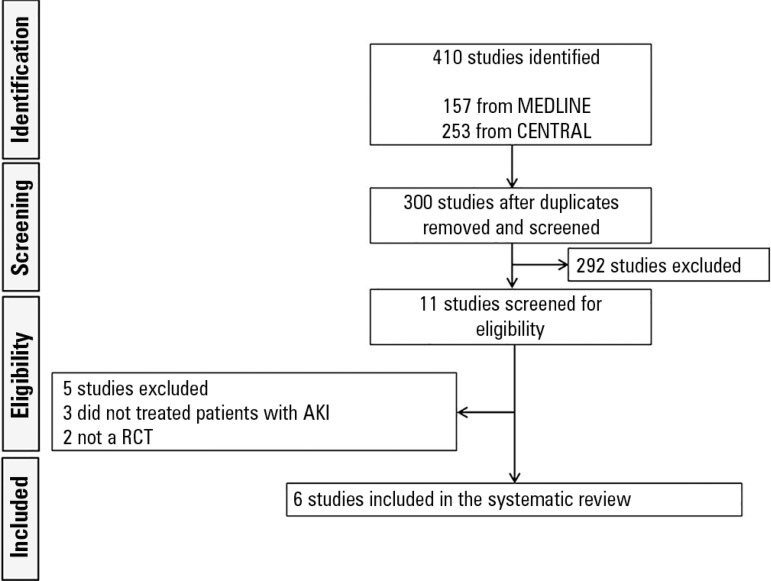
Methods: We performed a systematic review and meta-analysis of randomized controlled trials comparing early versus delayed initiation of renal replacement therapy in patients with acute kidney injury without the life-threatening acute kidney injury-related symptoms of fluid overload or metabolic disorders. Two investigators extracted the data from the selected studies. The Cochrane Risk of Bias Tool was used to assess the quality of the studies, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to test the overall quality of the evidence.
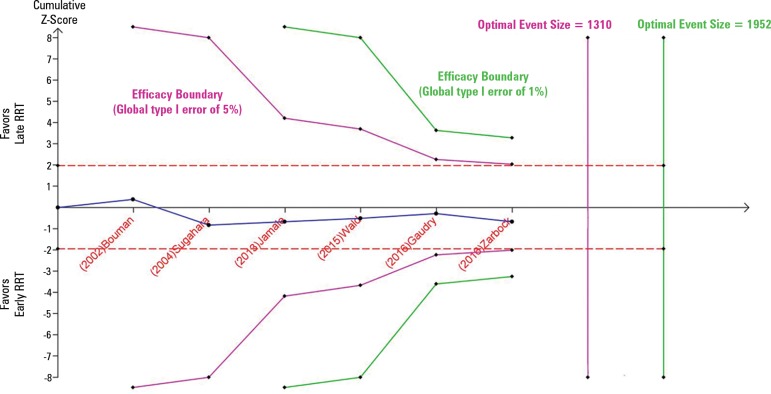
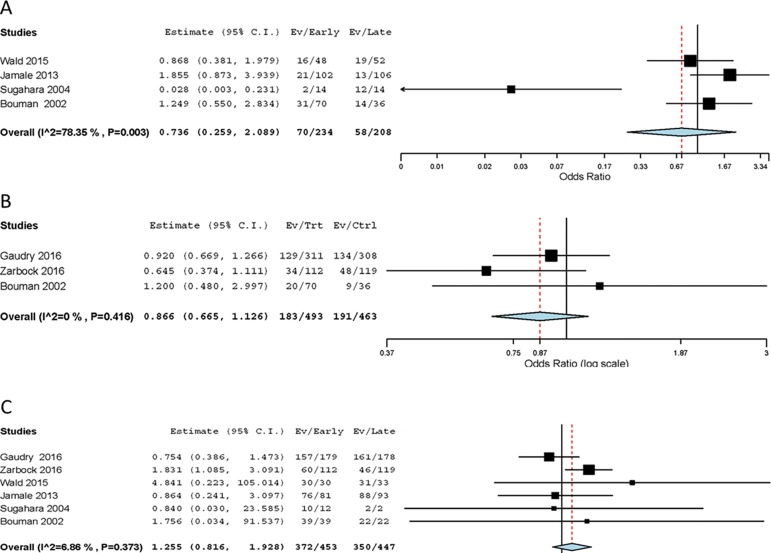
Results: Six randomized controlled trials (1,292 patients) were included. There was no statistically significant difference between early and delayed initiation of renal replacement therapy regarding the primary outcome (OR 0.82; 95%CI, 0.48 - 1.42; p = 0.488), but there was an increased risk of catheter-related bloodstream infection when renal replacement therapy was initiated early (OR 1.77; 95%CI, 1.01 - 3.11; p = 0.047). The quality of evidence generated by our meta-analysis for the primary outcome was considered low due to the risk of bias of the included studies and the heterogeneity among them.
Conclusion: Early initiation of renal replacement therapy is not associated with improved survival. However, the quality of the current evidence is low, and the criteria used for -early- and -delayed- initiation of renal replacement therapy are too heterogeneous among studies.
Objetivo: Avaliar se, em comparação ao início tardio, o início precoce da terapia de substituição renal se associa com menor mortalidade em pacientes com lesão renal aguda.
Métodos: Conduzimos uma revisão sistemática e metanálise de ensaios clínicos randomizados e controlados, que compararam terapia de substituição renal com início precoce àquela com início tardio em pacientes com lesão renal aguda, sem sintomas relacionados à insuficiência renal aguda que oferecessem risco à vida, como sobrecarga hídrica ou distúrbios metabólicos. Dois investigadores extraíram os dados a partir de estudos selecionados. Utilizaram-se a ferramenta Cochrane Risk of Bias, para avaliar a qualidade dos estudos, e a abordagem Grading of Recommendations Assessment, Development and Evaluation (GRADE), para testar a qualidade geral da evidência.
Resultados: Incluíram-se seis estudos clínicos randomizados e controlados (1.292 pacientes). Não houve diferença estatisticamente significante entre o início precoce e tardio da terapia de substituição renal, no que se referiu ao desfecho primário (OR 0,82; IC95% 0,48 - 1,42; p = 0,488). Foi maior o risco de infecção da corrente sanguínea relacionada ao cateter quando a terapia de substituição renal foi iniciada precocemente (OR 1,77; IC95% 1,01 - 3,11; p = 0,047). A qualidade da evidência gerada por nossa metanálise para o desfecho primário foi considerada baixa, em razão do risco de viés dos estudos incluídos e da heterogeneidade entre eles.
Conclusão: O início precoce da terapia de substituição renal não se associou com melhora da sobrevivência. Entretanto, a qualidade da evidência atual é baixa, e os critérios utilizados para início precoce e tardio da terapia de substituição renal foram demasiadamente heterogêneos entre os estudos.
Conflict of interest statement
Figures

References
-
- Tolwani A. Continuous renal-replacement therapy for acute kidney injury. N Engl J Med. 2012;367(26):2505–2514. - PubMed
-
- Villa G, Ricci Z, Ronco C. Renal replacement therapy. Crit Care Clin. 2015;31(4):839–848. - PubMed
-
- KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(Suppl):1–138.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
