

Maribavir for Refractory or Resistant Cytomegalovirus Infections in Hematopoietic-cell or Solid-organ Transplant Recipients: A Randomized, Dose-ranging, Double-blind, Phase 2 Study
- PMID: 30329038
- PMCID: PMC6451997
- DOI: 10.1093/cid/ciy706
Maribavir for Refractory or Resistant Cytomegalovirus Infections in Hematopoietic-cell or Solid-organ Transplant Recipients: A Randomized, Dose-ranging, Double-blind, Phase 2 Study
Abstract
Background: Cytomegalovirus (CMV) infections that are refractory or resistant (RR) to available antivirals ([val]ganciclovir, foscarnet, cidofovir) are associated with higher mortality in transplant patients. Maribavir is active against RR CMV strains.
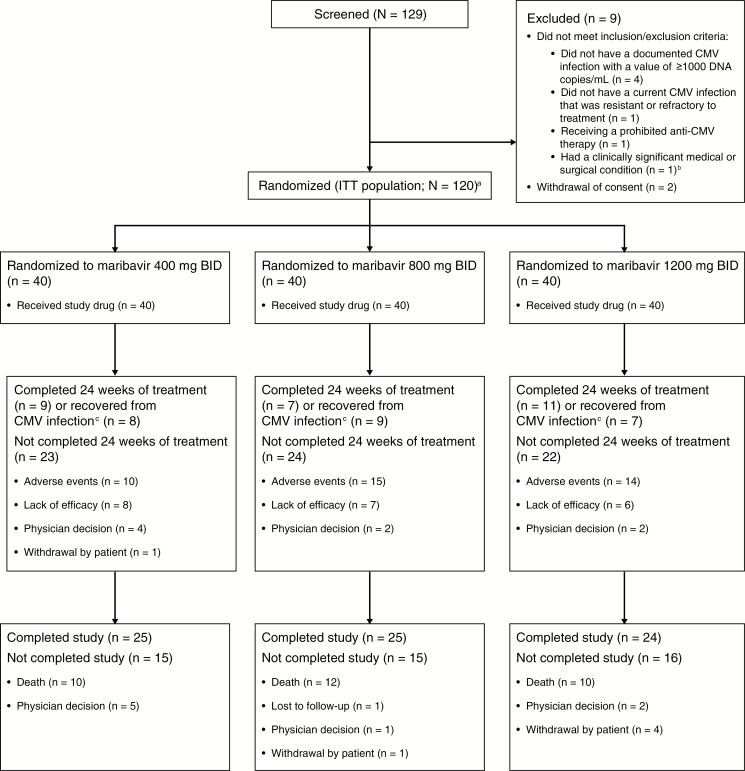
Methods: Hematopoietic-cell or solid-organ transplant recipients ≥12 years old with RR CMV infections and plasma CMV deoxyribonucleic acid (DNA) ≥1000 copies/mL were randomized (1:1:1) to twice-daily dose-blinded maribavir 400, 800, or 1200 mg for up to 24 weeks. The primary efficacy endpoint was the proportion of patients with confirmed undetectable plasma CMV DNA within 6 weeks of treatment. Safety analyses included the frequency and severity of treatment-emergent adverse events (TEAEs).
Results: From July 2012 to December 2014, 120 patients were randomized and treated (40 per dose group): 80/120 (67%) patients achieved undetectable CMV DNA within 6 weeks of treatment (95% confidence interval, 57-75%), with rates of 70%, 63%, and 68%, respectively, for maribavir 400, 800, and 1200 mg twice daily. Recurrent on-treatment CMV infections occurred in 25 patients; 13 developed mutations conferring maribavir resistance. Maribavir was discontinued due to adverse events in 41/120 (34%) patients, and 17/41 discontinued due to CMV infections. During the study, 32 (27%) patients died, 4 due to CMV disease. Dysgeusia was the most common TEAE (78/120; 65%) and led to maribavir discontinuation in 1 patient. Absolute neutrophil counts <1000/µL were noted in 12/106 (11%) evaluable patients, with rates similar across doses.
Conclusions: Maribavir ≥400 mg twice daily was active against RR CMV infections in transplant recipients; no new safety signals were identified.
Clinical trials registration: NCT01611974.
Keywords: cytomegalovirus; foscarnet; ganciclovir; maribavir; transplantation.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures

References
-
- Limaye AP, Corey L, Koelle DM, Davis CL, Boeckh M. Emergence of ganciclovir-resistant cytomegalovirus disease among recipients of solid-organ transplants. Lancet 2000; 356:645–9. - PubMed
-
- Liu J, Kong J, Chang YJ, et al. . Patients with refractory cytomegalovirus (CMV) infection following allogeneic haematopoietic stem cell transplantation are at high risk for CMV disease and non-relapse mortality. Clin Microbiol Infect 2015; 21:1121.e9–15. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
