

The hidden burden of measles in Ethiopia: how distance to hospital shapes the disease mortality rate
- PMID: 30333039
- PMCID: PMC6193289
- DOI: 10.1186/s12916-018-1171-y
The hidden burden of measles in Ethiopia: how distance to hospital shapes the disease mortality rate
Abstract
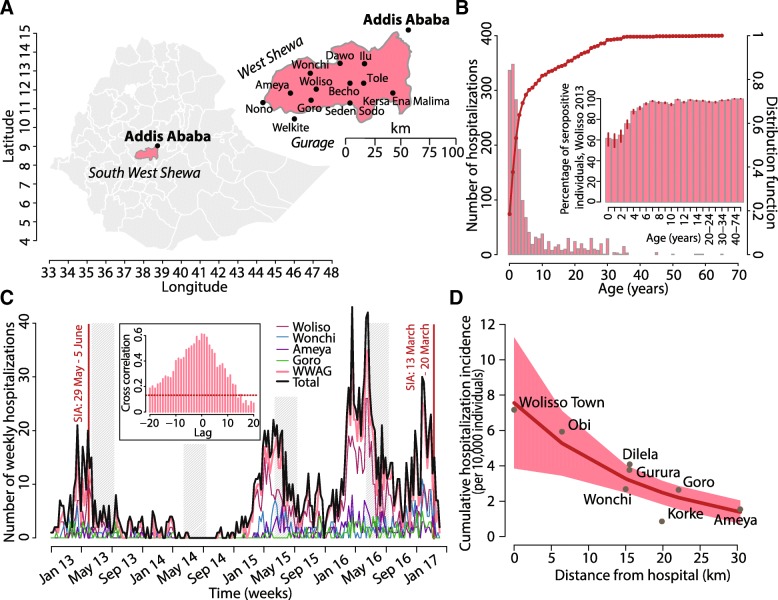
Background: A sequence of annual measles epidemics has been observed from January 2013 to April 2017 in the South West Shoa Zone of the Oromia Region, Ethiopia. We aimed at estimating the burden of disease in the affected area, taking into account inequalities in access to health care due to travel distances from the nearest hospital.
Methods: We developed a dynamic transmission model calibrated on the time series of hospitalized measles cases. The model provided estimates of disease transmissibility and incidence at a population level. Model estimates were combined with a spatial analysis to quantify the hidden burden of disease and to identify spatial heterogeneities characterizing the effectiveness of the public health system in detecting severe measles infections and preventing deaths.
Results: A total of 1819 case patients and 36 deaths were recorded at the hospital. The mean age was 6.0 years (range, 0-65). The estimated reproduction number was 16.5 (95% credible interval (CI) 14.5-18.3) with a cumulative disease incidence of 2.34% (95% CI 2.06-2.66). Three thousand eight hundred twenty-one (95% CI 1969-5671) severe cases, including 2337 (95% CI 716-4009) measles-related deaths, were estimated in the Woliso hospital's catchment area (521,771 inhabitants). The case fatality rate was found to remarkably increase with travel distance from the nearest hospital: ranging from 0.6% to more than 19% at 20 km. Accordingly, hospital treatment prevented 1049 (95% CI 757-1342) deaths in the area.
Conclusions: Spatial heterogeneity in the access to health care can dramatically affect the burden of measles disease in low-income settings. In sub-Saharan Africa, passive surveillance based on hospital admitted cases might miss up to 60% of severe cases and 98% of related deaths.
Keywords: Access to health care; Case fatality rate; Infectious diseases; Mathematical model; Measles epidemic; Sub-Saharan Africa.
Conflict of interest statement
Ethics approval and consent to participate
The study did not require informed consent as collected data consisted of routine health data and medical records were encrypted and anonymous and did not contain any information that might be used to identify individual patients.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Beyene BB, Tegegne AA, Wayessa DJ, Enqueselassie F. National measles surveillance data analysis, 2005 to 2009, Ethiopia. J Public Health Epidemiol. 2016;8:3.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
