

Can computer-aided diagnosis assist in the identification of prostate cancer on prostate MRI? a multi-center, multi-reader investigation
- PMID: 30333911
- PMCID: PMC6173466
- DOI: 10.18632/oncotarget.26100
Can computer-aided diagnosis assist in the identification of prostate cancer on prostate MRI? a multi-center, multi-reader investigation
Abstract
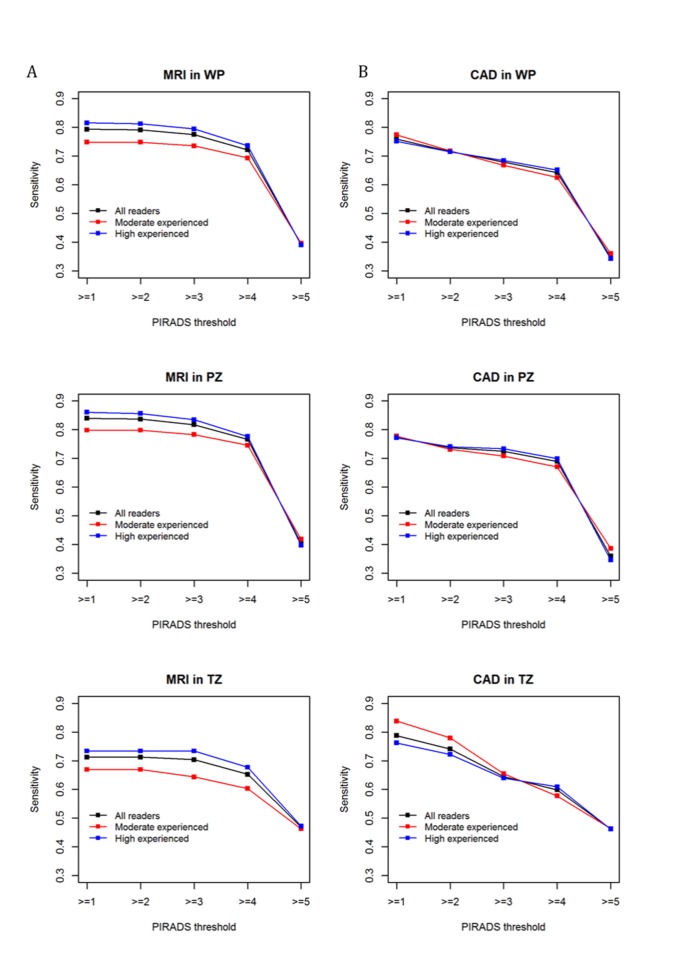
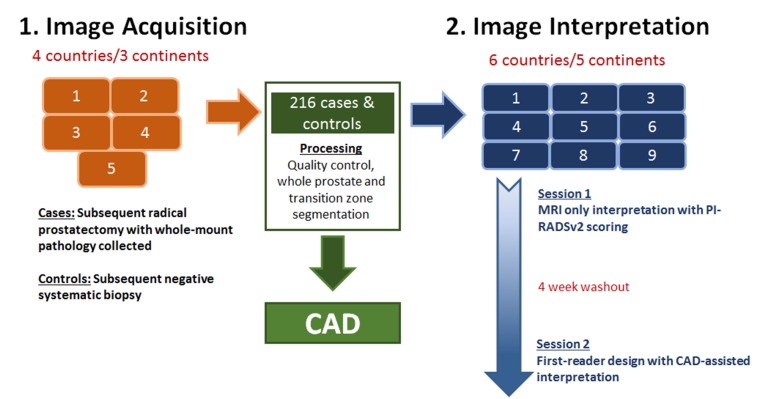
For prostate cancer detection on prostate multiparametric MRI (mpMRI), the Prostate Imaging-Reporting and Data System version 2 (PI-RADSv2) and computer-aided diagnosis (CAD) systems aim to widely improve standardization across radiologists and centers. Our goal was to evaluate CAD assistance in prostate cancer detection compared with conventional mpMRI interpretation in a diverse dataset acquired from five institutions tested by nine readers of varying experience levels, in total representing 14 globally spread institutions. Index lesion sensitivities of mpMRI-alone were 79% (whole prostate (WP)), 84% (peripheral zone (PZ)), 71% (transition zone (TZ)), similar to CAD at 76% (WP, p=0.39), 77% (PZ, p=0.07), 79% (TZ, p=0.15). Greatest CAD benefit was in TZ for moderately-experienced readers at PI-RADSv2 <3 (84% vs mpMRI-alone 67%, p=0.055). Detection agreement was unchanged but CAD-assisted read times improved (4.6 vs 3.4 minutes, p<0.001). At PI-RADSv2 ≥ 3, CAD improved patient-level specificity (72%) compared to mpMRI-alone (45%, p<0.001). PI-RADSv2 and CAD-assisted mpMRI interpretations have similar sensitivities across multiple sites and readers while CAD has potential to improve specificity and moderately-experienced radiologists' detection of more difficult tumors in the center of the gland. The multi-institutional evidence provided is essential to future prostate MRI and CAD development.
Keywords: PI-RADSv2; computer-aided diagnosis; multiparametric MRI; prostate cancer; tumor detection.
Conflict of interest statement
CONFLICTS OF INTEREST Dr. Ronald M. Summers: Patent royalties from iCAD & ScanMed, Research support from Ping An & NVidia, Software licenses to Philips & Ping An. Dr. Bradford J. Wood reports grants from NIH Intramural Research Program , during the conduct of the study; grants and non-financial support from CRADA with Philips, grants and non-financial support from CRADA with Celsion Corp, grants and non-financial support from CRADA with Siemens, grants and non-financial support from CRADA with Biocompatibles BTG, grants and non-financial support from CRADA with NVIDIA, grants and non-financial support from CRADA with Profound Medical, grants and non-financial support from CRADA with XAct Robotics, outside the submitted work; In addition, Dr. Wood has a patent Fusion Patents with royalties paid to NIH and to Dr. Wood by Philips, but this is unrelated to this work.
Figures
References
-
- Siddiqui MM, Rais-Bahrami S, Turkbey B, George AK, Rothwax J, Shakir N, Okoro C, Raskolnikov D, Parnes HL, Linehan WM, Merino MJ, Simon RM, Choyke PL, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. 2015;313:390–7. doi: 10.1001/jama.2014.17942. - DOI - PMC - PubMed
-
- Rais-Bahrami S, Siddiqui MM, Turkbey B, Stamatakis L, Logan J, Hoang AN, Walton-Diaz A, Vourganti S, Truong H, Kruecker J, Merino MJ, Wood BJ, Choyke PL, et al. Utility of multiparametric magnetic resonance imaging suspicion levels for detecting prostate cancer. J Urol. 2013;190:1721–7. doi: 10.1016/j.juro.2013.05.052. - DOI - PMC - PubMed
-
- Kasivisvanathan V, Rannikko AS, Borghi M, Panebianco V, Mynderse LA, Vaarala MH, Briganti A, Budaus L, Hellawell G, Hindley RG, Roobol MJ, Eggener S, Ghei M, et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med. 2018;378:1767–1777. doi: 10.1056/NEJMoa1801993. - DOI - PMC - PubMed
-
- Mehralivand S, Shih JH, Rais-Bahrami S, Oto A, Bednarova S, Nix JW, Thomas JV, Gordetsky JB, Gaur S, Harmon SA, Siddiqui MM, Merino MJ, Parnes HL, et al. A Magnetic Resonance Imaging-Based Prediction Model for Prostate Biopsy Risk Stratification. JAMA Oncol. 2018;4:678–685. doi: 10.1001/jamaoncol.2017.5667. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
