

Surgery Provides Long-Term Survival in Patients with Metastatic Neuroendocrine Tumors Undergoing Resection for Non-Hormonal Symptoms
- PMID: 30334178
- PMCID: PMC10183101
- DOI: 10.1007/s11605-018-3986-4
Surgery Provides Long-Term Survival in Patients with Metastatic Neuroendocrine Tumors Undergoing Resection for Non-Hormonal Symptoms
Abstract
Introduction: Patients with metastatic neuroendocrine tumor (NET) often have an indolent disease course yet the outcomes for patients with metastatic NET undergoing surgery for non-hormonal (NH) symptoms of GI obstruction, bleeding, or pain is not known.
Methods: We identified patients with metastatic gastroenteropancreatic NET who underwent resection from 2000 to 2016 at 8 academic institutions who participated in the US Neuroendocrine Tumor Study Group.
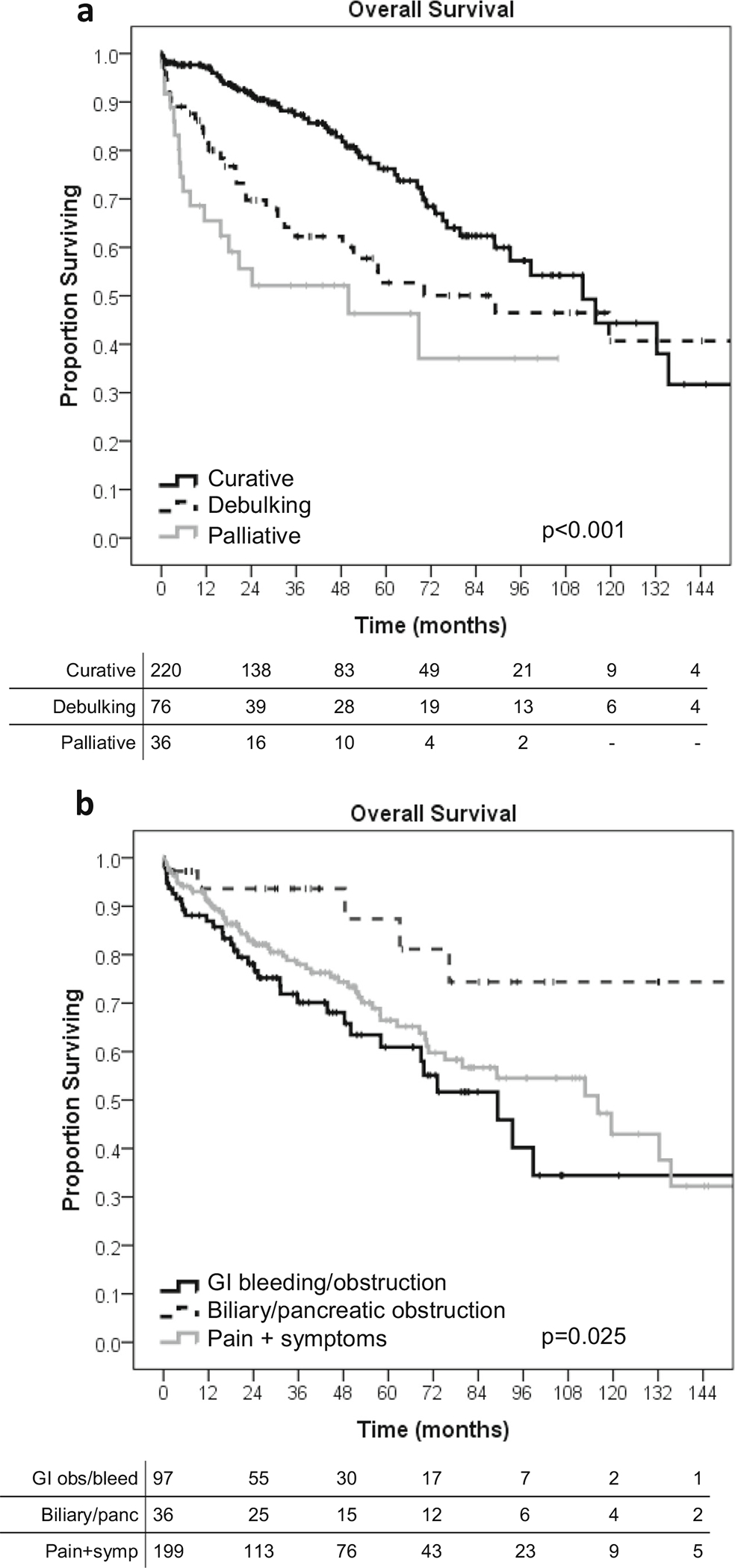
Results: Of 581 patients with metastatic NET to liver (61.3%), lymph nodes (24.1%), lung (2.1%), and bone (2.5%), 332 (57.1%) presented with NH symptoms of pain (n = 223, 67.4%), GI bleeding (n = 54, 16.3%), GI obstruction (n = 49, 14.8%), and biliary obstruction (n = 22, 6.7%). Most patients were undergoing their first operation (85.4%) within 4 weeks of diagnosis. The median overall survival was 110.4 months, and operative intent predicted survival (p < 0.001) with 66.3% undergoing curative resection. Removal of all metastatic disease was associated with the longest median survival (112.5 months) compared to debulking (89.2 months), or palliative resection (50.0 months; p < 0.001). The 1-, 3-, and 12-month mortality was 3.0%, 4.5%, and 9.0%, respectively. Factors associated with 1-year mortality included palliative operations (OR 6.54, p = 0.006), foregut NET (5.62, p = 0.042), major complication (4.91, p = 0.001), and high tumor grade (11.2, p < 0.001). The conditional survival for patients who lived past 1 year was 119 months.
Conclusions: Patients with metastatic NET and NH symptoms that necessitate surgery have long-term survival, and goals of care should focus on both oncologic and quality of life impact. Surgical intervention remains a critical component of multidisciplinary care of symptomatic patients.
Keywords: Metastatic; Neuroendocrine tumor; Non-hormonal; Palliative surgery; Symptoms.
Conflict of interest statement
Figures



Similar articles
-
Influence of carcinoid syndrome on the clinical characteristics and outcomes of patients with gastroenteropancreatic neuroendocrine tumors undergoing operative resection.Surgery. 2019 Mar;165(3):657-663. doi: 10.1016/j.surg.2018.09.008. Epub 2018 Oct 28. Surgery. 2019. PMID: 30377003 Free PMC article.
-
Outcomes of Cytoreductive Surgery for Metastatic Low-Grade Neuroendocrine Tumors in the Setting of Extrahepatic Metastases.Ann Surg Oncol. 2018 Jun;25(6):1768-1774. doi: 10.1245/s10434-018-6433-6. Epub 2018 Mar 20. Ann Surg Oncol. 2018. PMID: 29560571
-
Resection of primary tumor may prolong survival in metastatic gastroenteropancreatic neuroendocrine tumors.Surgery. 2019 Mar;165(3):644-651. doi: 10.1016/j.surg.2018.09.006. Epub 2018 Oct 23. Surgery. 2019. PMID: 30366604
-
Surgical management of neuroendocrine tumors.Best Pract Res Clin Endocrinol Metab. 2016 Jan;30(1):93-102. doi: 10.1016/j.beem.2015.10.003. Epub 2015 Oct 8. Best Pract Res Clin Endocrinol Metab. 2016. PMID: 26971846 Review.
-
GEP-NETS update: a review on surgery of gastro-entero-pancreatic neuroendocrine tumors.Eur J Endocrinol. 2014 Oct;171(4):R153-62. doi: 10.1530/EJE-14-0173. Epub 2014 Jun 11. Eur J Endocrinol. 2014. PMID: 24920289 Review.
Cited by
-
Metastatic MEN1 Syndrome Treated with Lutetium-177 - A Case Report.Eur Endocrinol. 2019 Aug;15(2):92-94. doi: 10.17925/EE.2019.15.2.92. Epub 2019 Aug 16. Eur Endocrinol. 2019. PMID: 31616499 Free PMC article.
-
Surgical resection of the primary tumor leads to prolonged survival in metastatic pancreatic neuroendocrine carcinoma.World J Surg Oncol. 2019 Mar 21;17(1):54. doi: 10.1186/s12957-019-1597-5. World J Surg Oncol. 2019. PMID: 30898132 Free PMC article.
-
Resection of the Primary Tumor Improves the Survival of Patients With Stage IV Gastric Neuroendocrine Carcinoma.Front Oncol. 2022 Jul 14;12:930491. doi: 10.3389/fonc.2022.930491. eCollection 2022. Front Oncol. 2022. PMID: 35912176 Free PMC article.
-
Role of surgical treatments in high-grade or advanced gastroenteropancreatic neuroendocrine neoplasms.World J Gastrointest Surg. 2022 May 27;14(5):397-408. doi: 10.4240/wjgs.v14.i5.397. World J Gastrointest Surg. 2022. PMID: 35734618 Free PMC article. Review.
-
Palliative surgery: state of the science and future directions.Br J Surg. 2024 Mar 2;111(3):znae068. doi: 10.1093/bjs/znae068. Br J Surg. 2024. PMID: 38502548 Free PMC article.
References
-
- Frilling A, Modlin IM, Kidd M, et al. Recommendations for management of patients with neuroendocrine liver metastases. Lancet Oncol. 2014;15(1):e8–21. - PubMed
-
- Pavel M, O’Toole D, Costa F, et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology. 2016;103(2):172–185. - PubMed
-
- Boudreaux JP, Klimstra DS, Hassan MM, et al. The NANETS consensus guideline for the diagnosis and management of neuroendocrine tumors: well-differentiated neuroendocrine tumors of the Jejunum, Ileum, Appendix, and Cecum. Pancreas. 2010;39(6): 753–766. - PubMed
-
- Rinke A, Muller HH, Schade-Brittinger C, et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group. J Clin Oncol. 2009;27(28):4656–4663. - PubMed
-
- Caplin ME, Pavel M, Cwikla JB, et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N Engl J Med. 2014;371(3):224–233. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
