

Angio-Computed Tomograph-Guided Immediate Lipiodol Computed Tomograph for Diagnosis of Small Hepatocellular Carcinoma Lesions during Transarterial Chemoembolization
- PMID: 30334525
- PMCID: PMC6202594
- DOI: 10.4103/0366-6999.243554
Angio-Computed Tomograph-Guided Immediate Lipiodol Computed Tomograph for Diagnosis of Small Hepatocellular Carcinoma Lesions during Transarterial Chemoembolization
Abstract
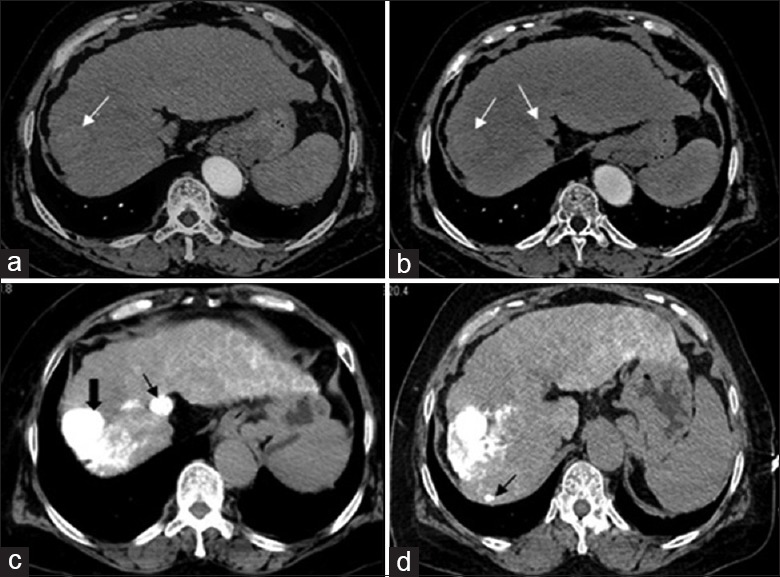
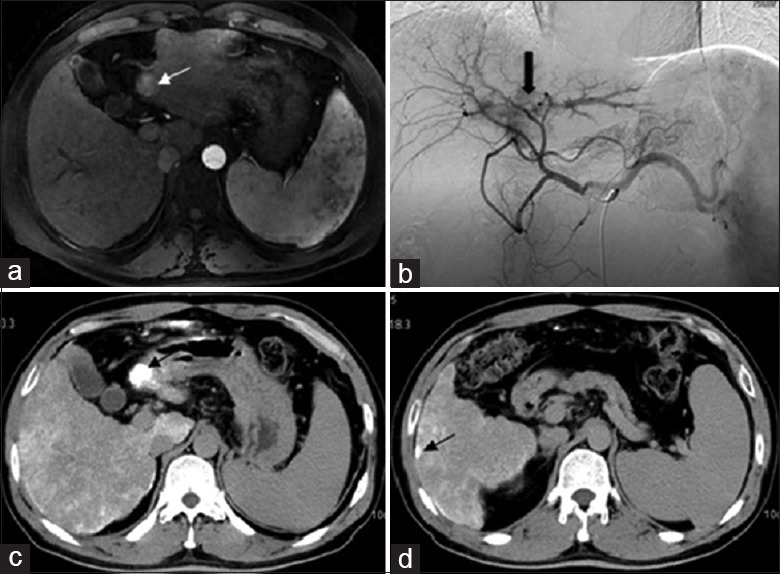
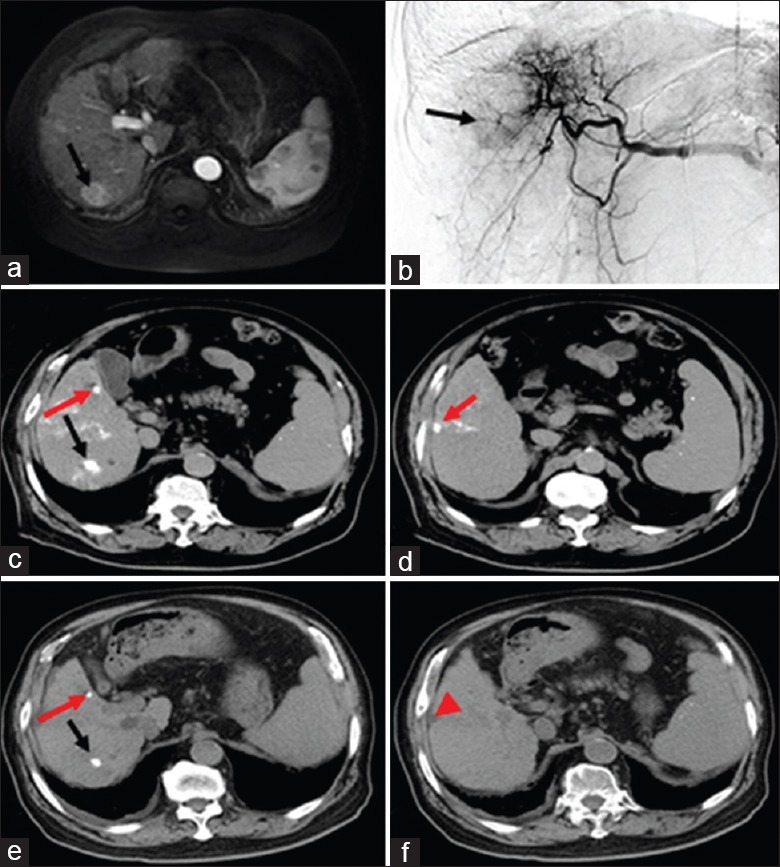
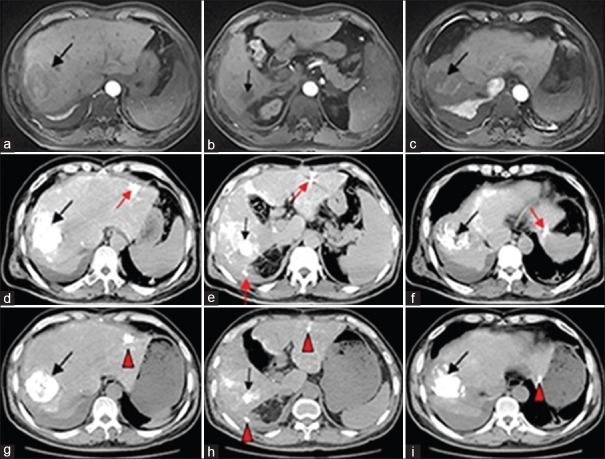
Background: The diagnosis and treatment of small hepatocellular carcinoma (HCC) play a vital role in the prognosis of patients with HCC. The purpose of our study was to evaluate angio-computed tomography (angio-CT)-guided immediate lipiodol CT (a CT scan performed immediately after transarterial chemoembolization [TACE]) in the diagnosis of potential HCCs ≤1 cm in diameter.
Methods: This study retrospectively analyzed 31 patients diagnosed with HCCs after routine imaging (contrast-enhanced CT or magnetic resonance imaging) or pathologic examinations with undefined or undetermined tumor lesions (diameter ≤1 cm) from February 2016 to September 2016. After TACE guided by digital subtraction angiography of the angio-CT system, potential HCC lesions with a diameter ≤1 cm were diagnosed by immediate lipiodol CT. The number of well-demarcated lesions was recorded to calculate the true positive rate. The correlation between the number of small HCCs detected by immediate lipiodol CT and the size of HCC lesions (diameter >1 cm) diagnosed preoperatively was analyzed 1 month after TACE. A paired t-test was used to analyze differences in liver function. Pearson analysis was used to analyze correlation. Chi-square test was used to compare the rates.
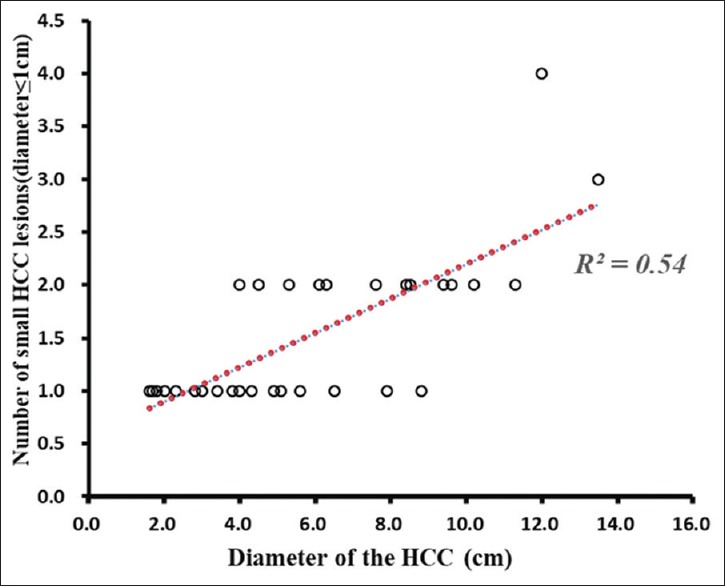
Results: Fifty-eight lesions were detected on preoperative routine imaging examinations in 31 patients including 15 lesions with a diameter ≤1 cm. Ninety-one lesions were detected on immediate lipiodol CT, of which 48 had a diameter ≤1 cm. After 1 month, CT showed that 45 lesions had lipiodol deposition and three lesions had lipiodol clearance. Correlation analysis showed that the number of small HCCs detected by lipiodol CT was positively correlated with the size of HCC lesions diagnosed by conventional imaging examination (R2 = 0.54, P < 0.05).
Conclusion: Immediate lipiodol CT may be a useful tool in the diagnosis of potential HCC lesions with a diameter of ≤1 cm.
Angio-CT引导经动脉化疗栓塞术后行即刻碘油CT成像诊断微小肝癌的临床研究 摘要 背景:微小肝癌的诊断和治疗对于肝癌(HCC)患者的预后有至关重要的作用。该研究的目的是探讨angio-CT引导的即刻碘油CT即angio-CT引导下行经动脉化疗栓塞(TACE)后即刻行CT扫描在诊断微小肝癌(≤1cm)中的应用价值。 方法:回顾性分析2016年2月至2016年9月在常规影像学检查(增强CT或增强 MRI)或病理学检查中未确诊或未发现的31例伴有微小肝癌(直径≤1cm)的HCC患者。于angio-CT系统的数字减影血管造影(digital subtraction angiograph, DSA)引导下行TACE治疗,术后即刻行CT扫描。记录边界清楚,碘油沉积良好的病灶数量。TACE后1个月行CT检查,分别记录碘油沉积和碘油廓清的病灶数量。两组间比较采用配对t检验,相关性分析采用Pearson correlation分析,率的比较采用卡方检验。 结果:31例患者术前常规影像学检查共发现58个病灶,其中15个病灶直径≤1cm。即刻碘油CT发现91个病灶,其中48个病灶直径≤1cm。1个月后,CT检查提示即刻碘油CT发现的48个病灶中,45个病灶有碘油沉积,3个病灶出现碘油廓清。Pearson相关分析显示即刻碘油CT检测到的微小肝癌数量与已经确诊的HCC病灶大小呈正相关(R2 =0.54, P <0.05)。 结论:即刻碘油CT可能是诊断直径≤1cm HCC的一种灵敏性较高的影像检查方法。.
Keywords: Chemoembolization; Diagnostic Imaging; Hepatocellular Carcinoma; Lipiodol Computed Tomograph; Liver Neoplasms; Therapeutic.
Conflict of interest statement
There are no conflicts of interest
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. - PubMed
-
- Xu L, Peng ZW, Chen MS, Shi M, Zhang YJ, Guo RP, et al. Prognostic nomogram for patients with unresectable hepatocellular carcinoma after transcatheter arterial chemoembolization. J Hepatol. 2015;63:122–30. doi: 10.1016/j.jhep.2015.02.034. - PubMed
-
- Agarwal A, Yadav AK, Kumar A, Gupta S, Panwala HK, Redhu N, et al. Transarterial chemoembolization in unresectable hepatocellular carcinoma – Assessing the factors affecting the survival: An audit from a tertiary care center in Northern India. Indian J Gastroenterol. 2015;4:1–10. doi: 10.1007/s12664-015-0544-9. - PubMed
-
- Galle PR, Forner A, Llovet JM, Mazzaferro V, Piscaglia F, Raoul JL, et al. EASL Clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. doi: 10.1016/j.jhep.2018.03.019. - PubMed
-
- Li T, Fan J, Qin LX, Zhou J, Sun HC, Qiu SJ, et al. Risk factors, prognosis, and management of early and late intrahepatic recurrence after resection of primary clear cell carcinoma of the liver. Ann Surg Oncol. 2011;18:1955–63. doi: 10.1245/s10434-010-1540-z. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
