

Altered hemodynamics contribute to local but not remote functional connectivity disruption due to glioma growth
- PMID: 30334672
- PMCID: PMC6928560
- DOI: 10.1177/0271678X18803948
Altered hemodynamics contribute to local but not remote functional connectivity disruption due to glioma growth
Abstract
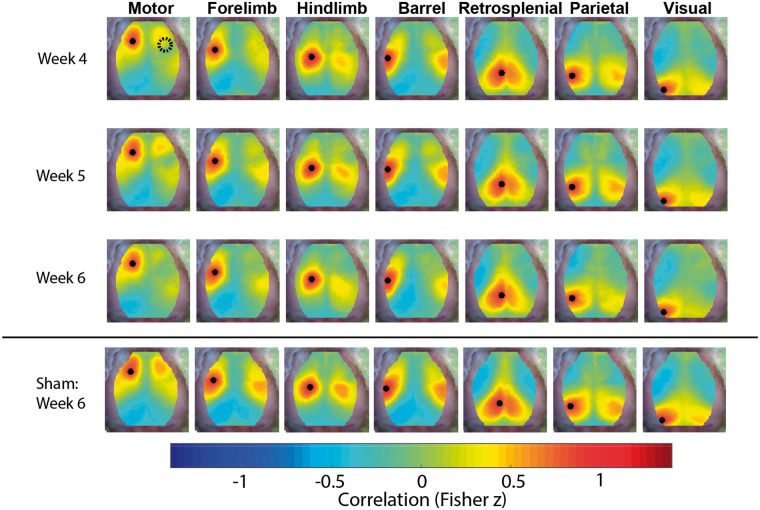
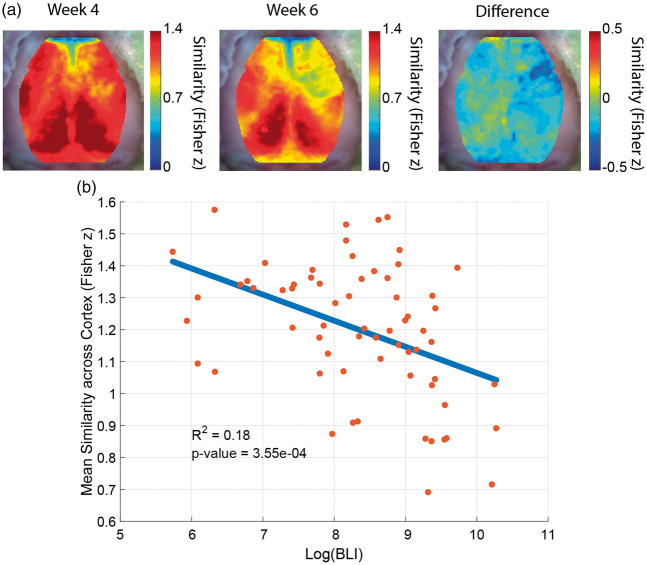
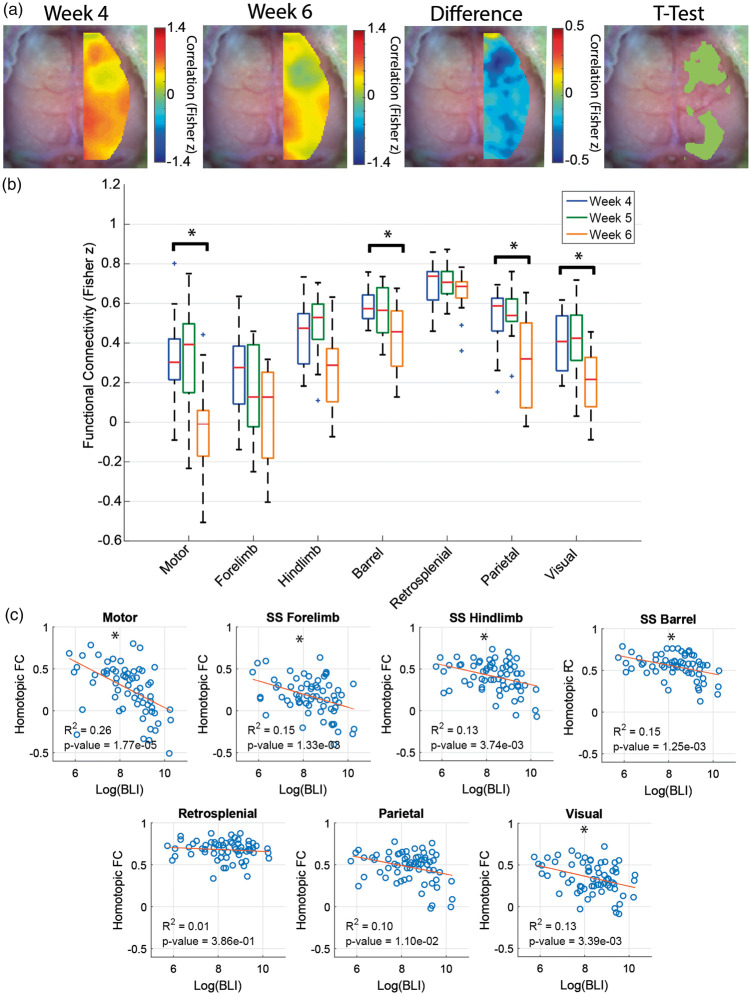
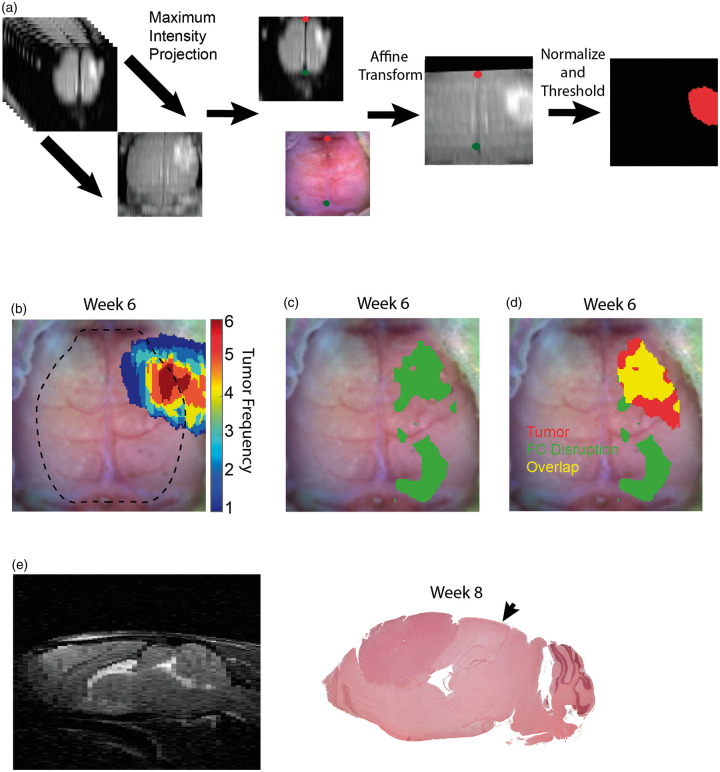
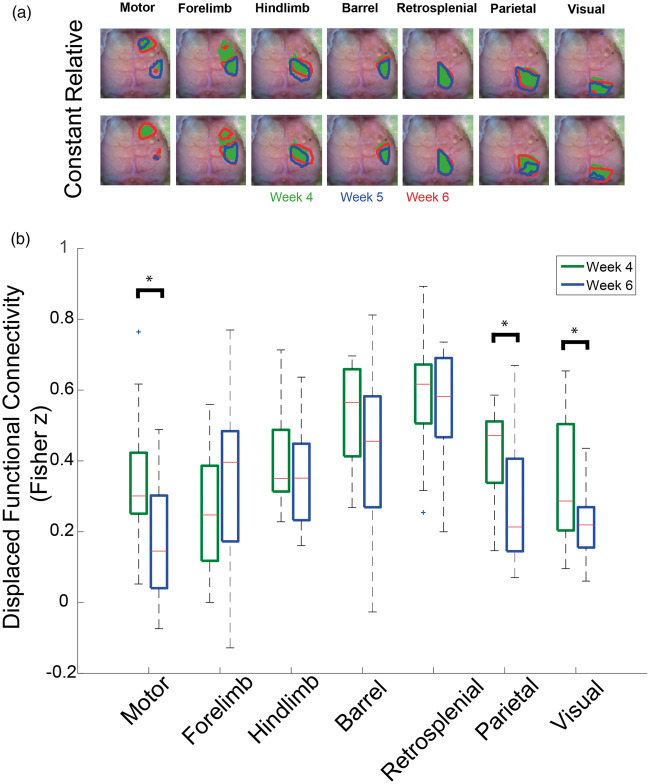
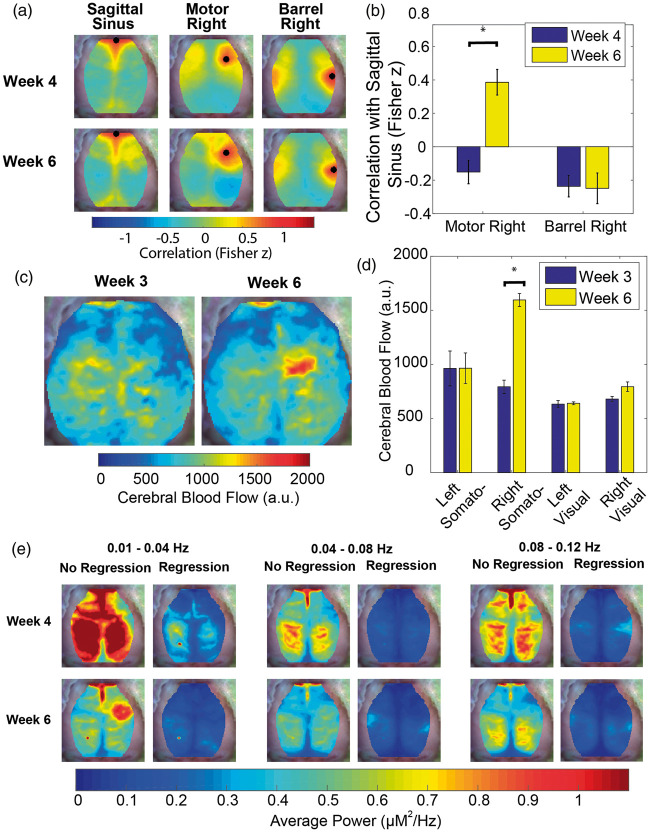
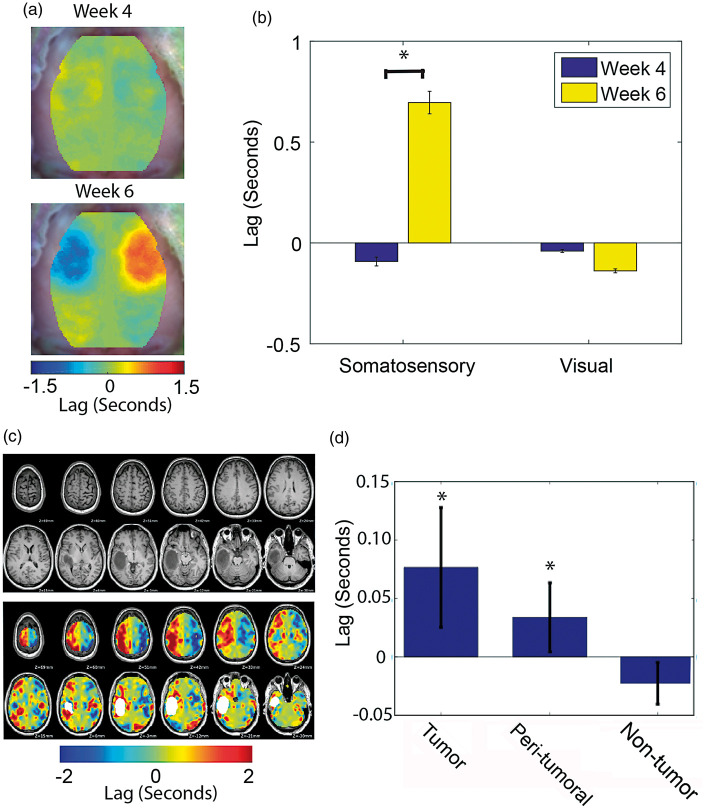
Glioma growth can cause pervasive changes in the functional connectivity (FC) of brain networks, which has been associated with re-organization of brain functions and development of functional deficits in patients. Mechanisms underlying functional re-organization in brain networks are not understood and efforts to utilize functional imaging for surgical planning, or as a biomarker of functional outcomes are confounded by the heterogeneity in available human data. Here we apply multiple imaging modalities in a well-controlled murine model of glioma with extensive validation using human data to explore mechanisms of FC disruption due to glioma growth. We find gliomas cause both local and distal changes in FC. FC changes in networks proximal to the tumor occur secondary to hemodynamic alterations but surprisingly, remote FC changes are independent of hemodynamic mechanisms. Our data strongly implicate hemodynamic alterations as the main driver of local changes in measurements of FC in patients with glioma.
Keywords: Functional connectivity; glioma; hemodynamic lags; mouse model; neurovascular uncoupling.
Figures
References
-
- Ghinda DC, Wu J-S, Duncan NW, et al. How much is enough – Can resting state fMRI provide a demarcation for neurosurgical resection in glioma?. Neurosci Biobehav Rev 2018; 84: 245–261. - PubMed
-
- Biswal B, Yetkin FZ, Haughton VM, et al. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med 1995; 34: 537–541. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
