

CT-guided special approaches of drainage for intraabdominal and pelvic abscesses: One single center's experience and review of literature
- PMID: 30335020
- PMCID: PMC6211865
- DOI: 10.1097/MD.0000000000012905
CT-guided special approaches of drainage for intraabdominal and pelvic abscesses: One single center's experience and review of literature
Abstract
Background: To explore the safety and efficacy of several special approaches of drainage for deep inaccessible intraabdominal and pelvic abscesses.
Methods: By searching of our institutional database, the clinical and radiologic information of all patients with special approaches of abscesses drainage was collected, consisting of etiology, diameter of abscess, duration of drainage, major complications, rates of success, failure and death, and pre-procedure, intra-procedure and post-procedure computed tomography scans.
Results: A total of 124 patients are eligible for the criterion in our center between January 2010 and January 2018. The mean diameter of abscess was 5.6 cm (range 3.0-9.8 cm) and mean duration of drainage was 10.3 days (range 4-43 days). Pain was complained in 6 patients (4.8%) and hemorrhage was observed in one patient. Complete resolution of the abscess following drainage was observed in 115 patients (92.7%). A total of 9 patients (7.3%) failed to percutaneous abscess drainage and 3 patients died of catheter-unrelated diseases. Transintestinal afferent loop of drainage was firstly attempted in six patients and complete resolution of abscess was achieved in five patients.
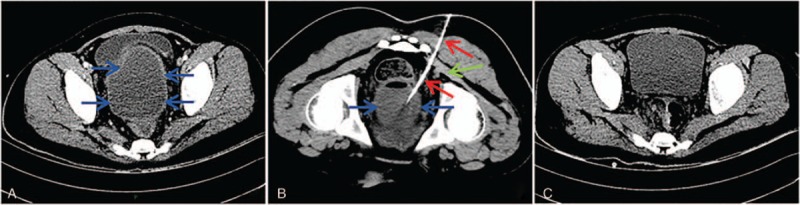
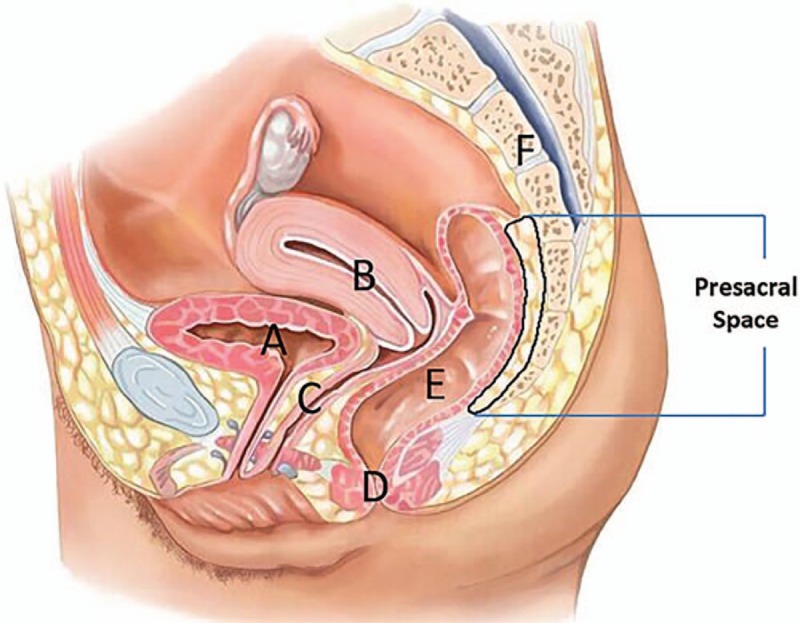
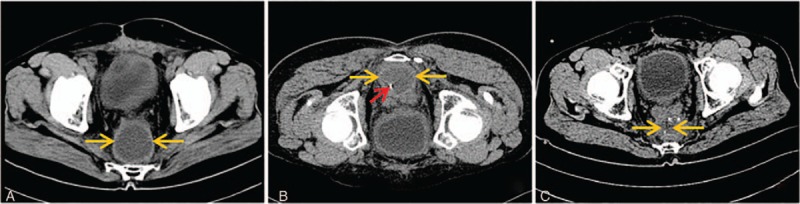
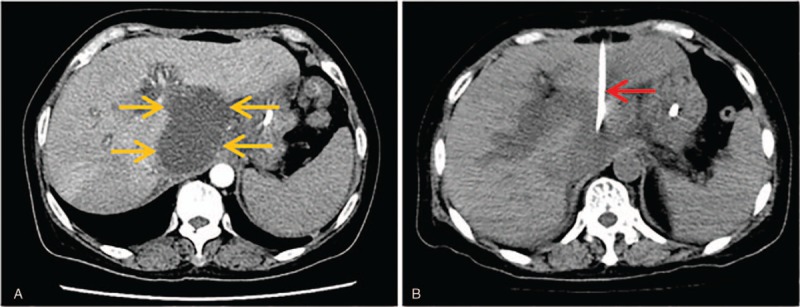
Conclusion: Special approaches, including transgluteal, presacral space, transhepatic, multiplane reconstruction (MPR)-assisted oblique approach and transintestinal afferent loop approach for those deep inaccessible intraabdominal and pelvic abscesses are safe and feasible.
Conflict of interest statement
The authors certify that they have no conflicts of interest to disclose.
Figures
Similar articles
-
CT-guided Drainage of Deep Pelvic Abscesses via a Percutaneous Presacral Space Approach: A Clinical Report and Review of the Literature.Acad Radiol. 2016 Dec;23(12):1553-1558. doi: 10.1016/j.acra.2016.06.009. Epub 2016 Oct 12. Acad Radiol. 2016. PMID: 27743740 Review.
-
Percutaneous transgluteal drainage of pelvic abscesses in interventional radiology: A safe alternative to surgery.J Visc Surg. 2016 Feb;153(1):3-7. doi: 10.1016/j.jviscsurg.2015.10.006. Epub 2015 Oct 27. J Visc Surg. 2016. PMID: 26522506
-
Percutaneous, computed tomography-guided drainage of deep pelvic abscesses via a transgluteal approach: a report on 30 cases and a review of the literature.Abdom Imaging. 2013 Apr;38(2):285-9. doi: 10.1007/s00261-012-9917-z. Abdom Imaging. 2013. PMID: 22684488 Review.
-
Transgluteal approach for percutaneous drainage of deep pelvic abscesses: 154 cases.Radiology. 2003 Sep;228(3):701-5. doi: 10.1148/radiol.2283020924. Epub 2003 Jul 24. Radiology. 2003. PMID: 12881584
-
[Analysis of the effect of transgluteal percutaneous drainage in the treatment of deep pelvic abscess].Zhonghua Wei Chang Wai Ke Za Zhi. 2020 Dec 25;23(12):1177-1181. doi: 10.3760/cma.j.cn.441530-20201103-00588. Zhonghua Wei Chang Wai Ke Za Zhi. 2020. PMID: 33353273 Chinese.
Cited by
-
Common Options and Overlooked Alternative for Drainage of Inaccessible Presacral Abscess: A Case Report.Acta Med Litu. 2021;28(1):170-175. doi: 10.15388/Amed.2021.28.1.13. Epub 2021 Mar 15. Acta Med Litu. 2021. PMID: 34393641 Free PMC article.
-
Accessing Intraabdominal Abscess for Percutaneous Drainage Using a Trocar Only Technique to Maneuver Intervening Bowel.Indian J Radiol Imaging. 2022 Dec 26;33(2):246-248. doi: 10.1055/s-0042-1759855. eCollection 2023 Apr. Indian J Radiol Imaging. 2022. PMID: 37123574 Free PMC article.
-
Indian College of Radiology and Imaging Consensus Guidelines on Interventions in Pancreatitis.Indian J Radiol Imaging. 2022 Jul 31;32(3):339-354. doi: 10.1055/s-0042-1754313. eCollection 2022 Sep. Indian J Radiol Imaging. 2022. PMID: 36177275 Free PMC article. Review.
-
Biliary injuries after pancreatic surgery: interventional radiology management.Gland Surg. 2019 Apr;8(2):141-149. doi: 10.21037/gs.2019.01.05. Gland Surg. 2019. PMID: 31183324 Free PMC article. Review.
-
Computerized tomography features acting as predictors for invasive therapy in the management of Crohn's disease-related spontaneous intra-abdominal abscess: experience from long-term follow-up.BMC Med Imaging. 2024 Nov 5;24(1):300. doi: 10.1186/s12880-024-01475-2. BMC Med Imaging. 2024. PMID: 39501173 Free PMC article.
References
-
- Ryan RS, McGrath FP, Haslam PJ, et al. Ultrasound-guided endocavitary drainage of pelvic abscesses: technique, results and complications. Clin Radiol 2003;58:75–9. - PubMed
-
- Hsu RB, Chen RJ, Wang SS, et al. Determinants of successful surgical revascularization for failed angioplasty in patients with acute myocardial infarction and cardiogenic shock. J Formos Med Assoc 2002;101:815–9. - PubMed
-
- Duszak RJ, Levy JM, Akins EW, et al. Percutaneous catheter drainage of infected intra-abdominal fluid collections. American College of Radiology. ACR Appropriateness Criteria. Radiology 2000;215suppl:1067–75. - PubMed
-
- Saokar A, Arellano RS, Gervais DA, et al. Transvaginal drainage of pelvic fluid collections: results, expectations, and experience. AJR Am J Roentgenol 2008;191:1352–8. - PubMed
