

Perceived Barriers to Mobility in a Medical ICU: The Patient Mobilization Attitudes & Beliefs Survey for the ICU
- PMID: 30336716
- PMCID: PMC6541532
- DOI: 10.1177/0885066618807120
Perceived Barriers to Mobility in a Medical ICU: The Patient Mobilization Attitudes & Beliefs Survey for the ICU
Abstract
Purpose: Early mobilization in the intensive care unit (ICU) can improve patient outcomes but has perceived barriers to implementation. As part of an ongoing structured quality improvement project to increase mobilization of medical ICU patients by nurses and clinical technicians, we adapted the existing, validated Patient Mobilization Attitudes & Beliefs Survey (PMABS) for the ICU setting and evaluated its performance characteristics and results.
Materials and methods: The 26-item PMABS adapted for the ICU (PMABS-ICU) was administered as an online survey to 163 nurses, clinical technicians, respiratory therapists, attending and fellow physicians, nurse practitioners, and physician assistants in one medical ICU. We evaluated the overall and subscale (knowledge, attitude, and behavior) scores and compared these scores by respondent characteristics (clinical role and years of work experience).
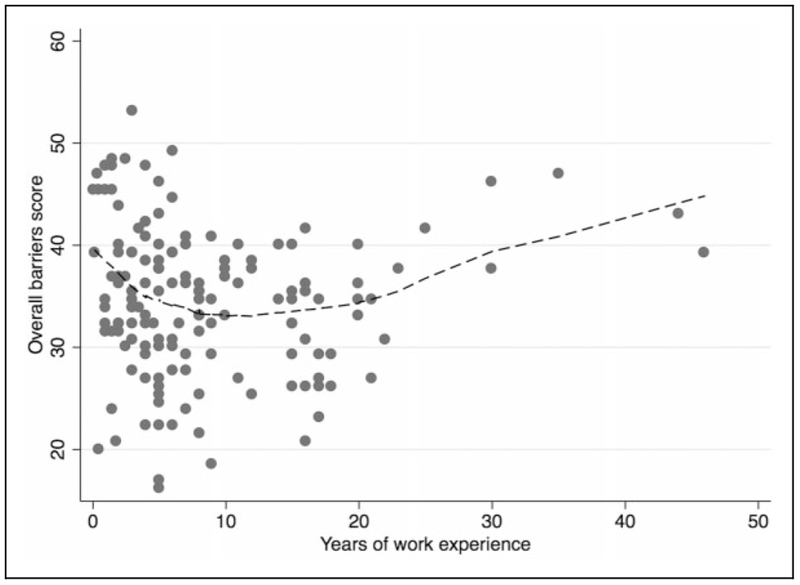
Results: The survey response rate was 96% (155/163). The survey demonstrated acceptable discriminant validity and acceptable internal consistency for the overall scale (Cronbach α: 0.82, 95% confidence interval: 0.76-0.85), with weaker internal consistency for all subscales (Cronbach α: 0.62-0.69). Across all respondent groups, the overall barrier score (range: 1-100) was relatively low, with attending physicians perceiving the lowest barriers (median [interquartile range]: 30 [28-34]) and nurses perceiving the highest (37 [31-40]). Within the first 10 years of work experience, greater experience was associated with a lower overall barrier score (-0.8 for each additional year; P = 0.02).
Conclusions: In our medical ICU, across 6 different clinical roles, there were relatively low perceived barriers to patient mobility, with greater work experience over the first 10 years being associated with lower perceived barriers. As part of a structured quality improvement project, the PMABS-ICU may be valuable in assisting to identify specific perceived barriers for consideration in designing mobility interventions for the ICU setting.
Keywords: barriers; early mobility; multiprofessional; quality improvement; rehabilitation; survey.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
