

Spinal Epidural Arteriovenous Fistula with Perimedullary Venous Reflux: Clinical and Neuroradiologic Features of an Underestimated Vascular Disorder
- PMID: 30337434
- PMCID: PMC7655362
- DOI: 10.3174/ajnr.A5854
Spinal Epidural Arteriovenous Fistula with Perimedullary Venous Reflux: Clinical and Neuroradiologic Features of an Underestimated Vascular Disorder
Abstract
Background and purpose: The purpose of this study was to discuss the clinical and radiologic characteristics of spinal epidural arteriovenous fistulas (SEAVF) and demonstrate their specific angiomorphology in a single-center series.
Materials and methods: Thirteen consecutive patients were diagnosed with SEAVF at RWTH Aachen University Hospital between 2006 and 2018 and were included in this study. All patients had MR imaging and DSA before treatment; 10 of these 13 patients received contrast-enhanced MRA (CE-MRA).
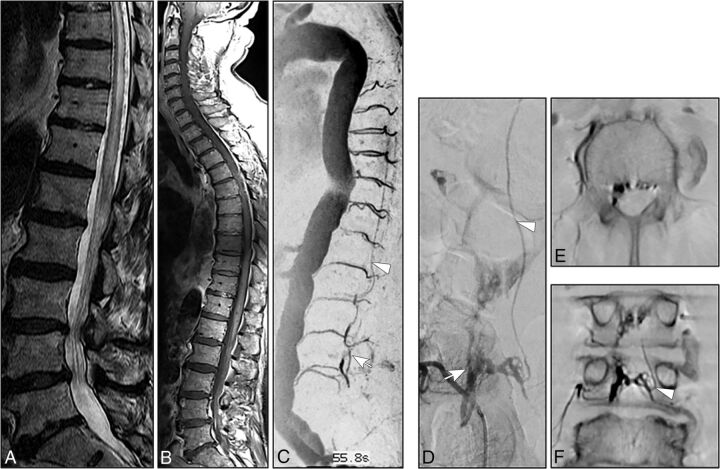
Results: The mean patient age was 72 ± 8 years. Paraparesis was present in 12 (92%) patients. Sphincter dysfunction and sensory symptoms were observed in 7 (54%) and 6 (46%) patients, respectively. The mean duration of symptoms was 6 ± 8 months. Congestive myelopathy on MR imaging was present in all patients. Prominent arterialized perimedullary veins were demonstrated in only 3 cases. CE-MRA revealed arterialized perimedullary veins and an arterialized epidural pouch in 9/10 (90%) patients, mostly located ventrolaterally. DSA demonstrated a multisegmental extension of the arterialized ventrolateral epidural pouch in 6 (46%) cases. An intradural radicular drainage vein was localized distant from the original fistula point in 3 (23%) patients.
Conclusions: Congestive myelopathy with an acute/subacute clinical course was the dominant finding in spinal epidural arteriovenous fistulas. CE-MRA is a powerful diagnostic tool for identifying arterialized perimedullary veins as well as an arterialized epidural pouch. While arterialized perimedullary veins frequently present with only mild enlargement and elongation in spinal epidural arteriovenous fistulas, the arterialized epidural pouch is frequently located ventrolaterally and may extend over several vertebral levels. DSA remains the criterion standard to precisely visualize a spinal epidural arteriovenous fistula and its intradural radicular drainage vein, which may be located distant from the fistulous point.
© 2018 by American Journal of Neuroradiology.
Figures


References
-
- Oldfield EH, Doppman JL. Spinal arteriovenous malformations. Clin Neurosurg 1988;34:161–83 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources