

Outcomes from stereotactic surgery for essential tremor
- PMID: 30337440
- PMCID: PMC6581115
- DOI: 10.1136/jnnp-2018-318240
Outcomes from stereotactic surgery for essential tremor
Abstract
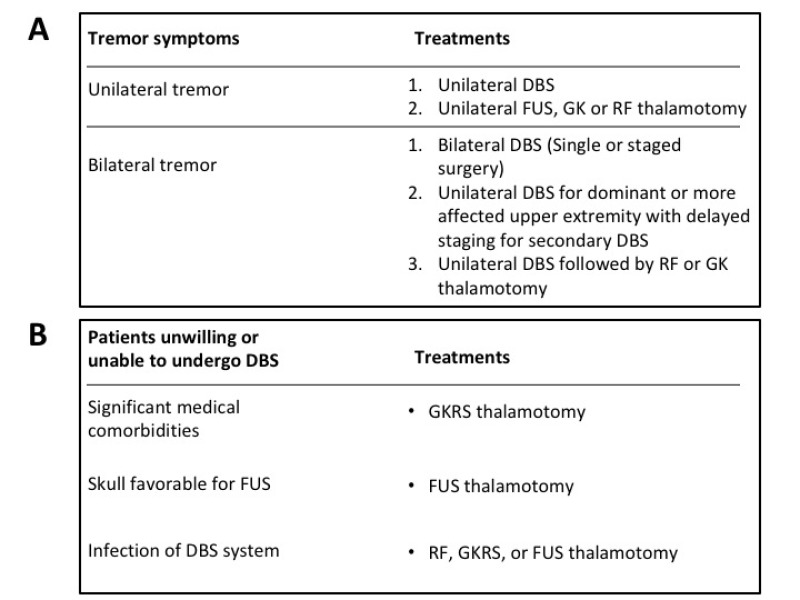
There are several different surgical procedures that are used to treat essential tremor (ET), including deep brain stimulation (DBS) and thalamotomy procedures with radiofrequency (RF), radiosurgery (RS) and most recently, focused ultrasound (FUS). Choosing a surgical treatment requires a careful presentation and discussion of the benefits and drawbacks of each. We conducted a literature review to compare the attributes and make an appraisal of these various procedures. DBS was the most commonly reported treatment for ET. One-year tremor reductions ranged from 53% to 63% with unilateral Vim DBS. Similar improvements were demonstrated with RF (range, 74%-90%), RS (range, 48%-63%) and FUS thalamotomy (range, 35%-75%). Overall, bilateral Vim DBS demonstrated more improvement in tremor reduction since both upper extremities were treated (range, 66%-78%). Several studies show continued beneficial effects from DBS up to five years. Long-term follow-up data also support RF and gamma knife radiosurgical thalamotomy treatments. Quality of life measures were similarly improved among patients who received all treatments. Paraesthesias, dysarthria and ataxia were commonly reported adverse effects in all treatment modalities and were more common with bilateral DBS surgery. Many of the neurological complications were transient and resolved after surgery. DBS surgery had the added benefit of programming adjustments to minimise stimulation-related complications. Permanent neurological complications were most commonly reported for RF thalamotomy. Thalamic DBS is an effective, safe treatment with a long history. For patients who are medically unfit or reluctant to undergo DBS, several thalamic lesioning methods have parallel benefits to unilateral DBS surgery. Each of these surgical modalities has its own nuance for treatment and patient selection. These factors should be carefully considered by both neurosurgeons and patients when selecting an appropriate treatment for ET.
Keywords: electrical stimulation; stereotaxic surgery; tremor; ultrasound.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: PDV has received grants for research from Research Fund Flanders (FWO) and the European Society for Stereotactic and Functional Neurosurgery (ESSFN) and grants for education and travel from the World Society of Stereotactic and Functional Neurosurgery (WSSFN), Medtronic and St. Jude-Abbott. AML is a consultant for Medtronic, Boston Scientific and Insightech. Alfonso Fasano is a consultant for Abbvie, Medtronic, Boston Scientific, Sunovion, Chiesi farmaceutici, UCB, Ipsen.
Figures
References
-
- Findley LJ. Epidemiology and genetics of essential tremor. Neurology 2000;54(Suppl 4):S8–S13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous