

Survival after radiation therapy for high-grade glioma
- PMID: 30337846
- PMCID: PMC6187089
- DOI: 10.1016/j.rpor.2018.09.003
Survival after radiation therapy for high-grade glioma
Abstract
Background: High-grade gliomas (HGGs) are a heterogeneous disease group, with variable prognosis, inevitably causing deterioration of the quality of life. The estimated 2-year overall survival is 20%, despite the best trimodality treatment consisting of surgery, chemotherapy, and radiotherapy.
Aim: To evaluate long-term survival outcomes and factors influencing the survival of patients with high-grade gliomas treated with radiotherapy.
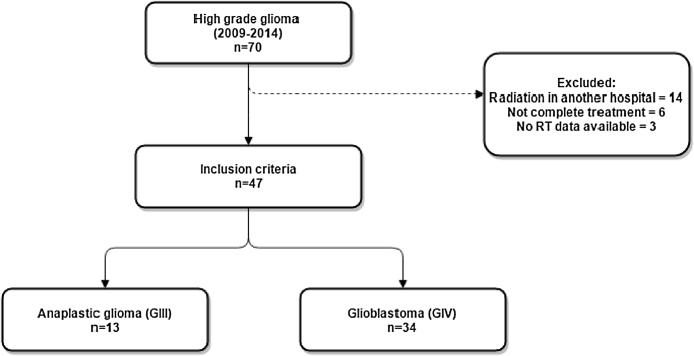
Materials and methods: Data from 47 patients diagnosed with high-grade gliomas between 2009 and 2014 and treated with three-dimensional radiotherapy (3DRT) or intensity-modulated radiotherapy (IMRT) were analyzed retrospectively.
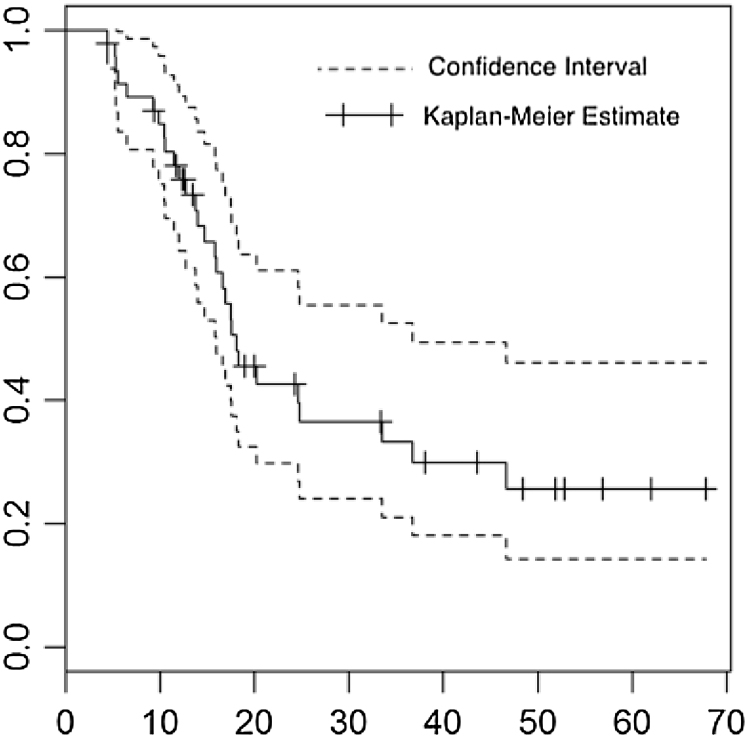
Results: Median survival was 16.6 months; 29 patients (62%) died before the time of analysis. IMRT was employed in 68% of cases. The mean duration of radiotherapy was 56 days, and the mean delay to the start of radiotherapy was 61.7 days (range, 27-123 days). There were no statistically significant effects of duration of radiotherapy or delay to the start of radiotherapy on patient outcomes.
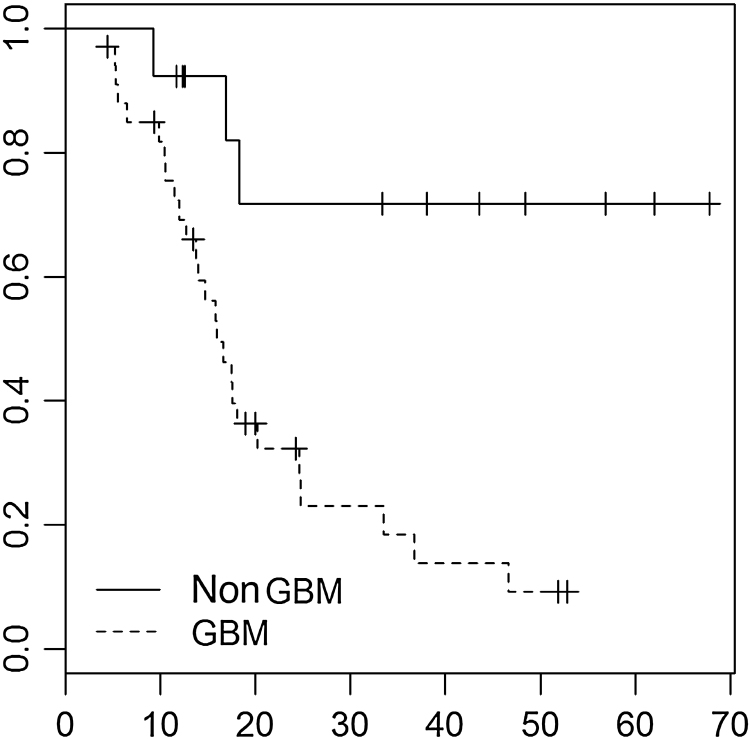
Conclusions: Age, total amount of gross resection, histological type, and use of adjuvant temozolomide influenced survival rate (p < 0.05). The estimated overall survival was 18 months (Kaplan-Meier estimator). Our results corroborated those reported in the literature.
Keywords: Anaplastic; Chemotherapy; Glioblastoma; Glioma; Radiotherapy.
Figures
References
-
- Wen P.Y., Macdonald D.R., Reardon D.A. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J Clin Oncol. 2010;28(11):1963–1972. - PubMed
-
- Caroline I., Rosenthal M.A. Imaging modalities in high-grade gliomas: pseudoprogression, recurrence, or necrosis? J Clin Neurosci. 2012;19(5):633–637. - PubMed
-
- Jahangiri A., Aghi M.K. Pseudoprogression and treatment effect. Neurosurg Clin N Am. 2012;23(2):277–287. - PubMed
-
- Stupp R., Mason W.P., van den Bent M.J. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
LinkOut - more resources
Full Text Sources
