

Cognitive Flexibility Predicts PTSD Symptoms: Observational and Interventional Studies
- PMID: 30337890
- PMCID: PMC6180246
- DOI: 10.3389/fpsyt.2018.00477
Cognitive Flexibility Predicts PTSD Symptoms: Observational and Interventional Studies
Abstract
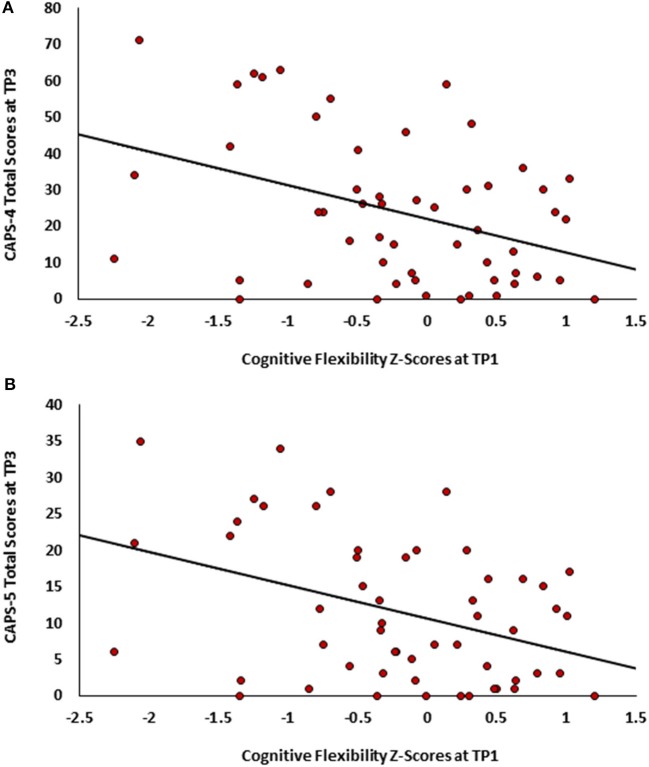
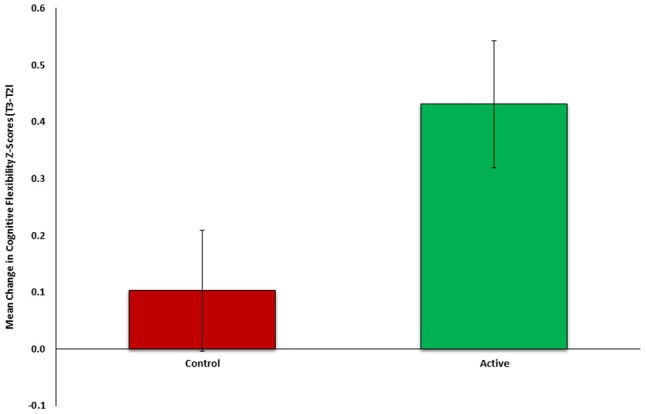
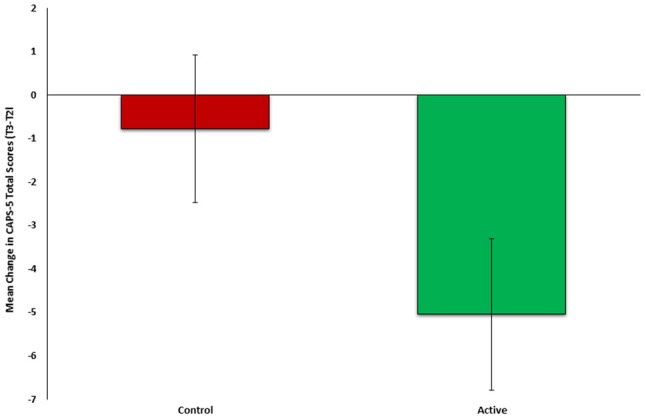
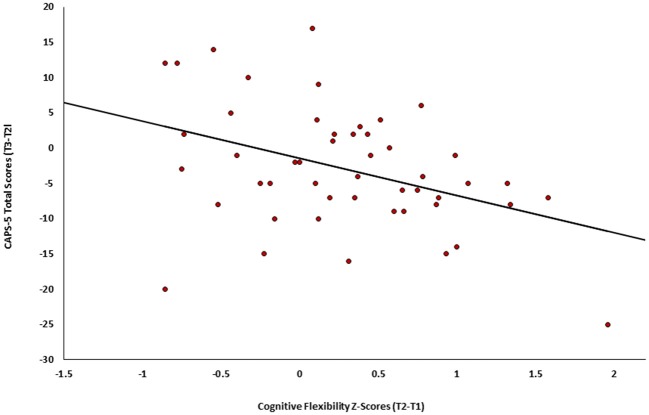
Introduction: Post-Traumatic Stress Disorder (PTSD) is a prevalent, severe and tenacious psychopathological consequence of traumatic events. Neurobehavioral mechanisms underlying PTSD pathogenesis have been identified, and may serve as risk-resilience factors during the early aftermath of trauma exposure. Longitudinally documenting the neurobehavioral dimensions of early responses to trauma may help characterize survivors at risk and inform mechanism-based interventions. We present two independent longitudinal studies that repeatedly probed clinical symptoms and neurocognitive domains in recent trauma survivors. We hypothesized that better neurocognitive functioning shortly after trauma will be associated with less severe PTSD symptoms a year later, and that an early neurocognitive intervention will improve cognitive functioning and reduce PTSD symptoms. Methods: Participants in both studies were adult survivors of traumatic events admitted to two general hospitals' emergency departments (EDs) in Israel. The studies used identical clinical and neurocognitive tools, which included assessment of PTSD symptoms and diagnosis, and a battery of neurocognitive tests. The first study evaluated 181 trauma-exposed individuals one-, six-, and 14 months following trauma exposure. The second study evaluated 97 trauma survivors 1 month after trauma exposure, randomly allocated to 30 days of web-based neurocognitive intervention (n = 50) or control tasks (n = 47), and re-evaluated all subjects three- and 6 months after trauma exposure. Results: In the first study, individuals with better cognitive flexibility at 1 month post-trauma showed significantly less severe PTSD symptoms after 13 months (p = 0.002). In the second study, the neurocognitive training group showed more improvement in cognitive flexibility post-intervention (p = 0.019), and lower PTSD symptoms 6 months post-trauma (p = 0.017), compared with controls. Intervention- induced improvement in cognitive flexibility positively correlated with clinical improvement (p = 0.002). Discussion: Cognitive flexibility, shortly after trauma exposure, emerged as a significant predictor of PTSD symptom severity. It was also ameliorated by a neurocognitive intervention and associated with a better treatment outcome. These findings support further research into the implementation of mechanism-driven neurocognitive preventive interventions for PTSD.
Keywords: Post-Traumatic Stress Disorder (PTSD); cognitive flexibility; cognitive training intervention; neurocognitive functioning; resilience factors; risk factors.
Figures
References
-
- Galatzer-Levy IR, Ankri Y, Freedman S, Israeli-Shalev Y, Roitman P, Gilad M, et al. . Early PTSD symptom trajectories: persistence, recovery, and response to treatment: results from the jerusalem trauma outreach and prevention study (J-TOPS). PLoS ONE (2013) 8:e70084. 10.1371/journal.pone.0070084 - DOI - PMC - PubMed
-
- Perkonigg A, Pfister H, Stein MB, Höfler M, Lieb R, Maercker A, et al. . longitudinal course of posttraumatic stress disorder and posttraumatic stress disorder symptoms in a community sample of adolescents and young adults. Am J Psychiatry (2005) 162:1320–7. 10.1176/appi.ajp.162.7.1320 - DOI - PubMed
LinkOut - more resources
Full Text Sources