

The Relationship Between Medial Gastrocnemius Lengthening Properties and Stretch Reflexes in Cerebral Palsy
- PMID: 30338247
- PMCID: PMC6180247
- DOI: 10.3389/fped.2018.00259
The Relationship Between Medial Gastrocnemius Lengthening Properties and Stretch Reflexes in Cerebral Palsy
Abstract
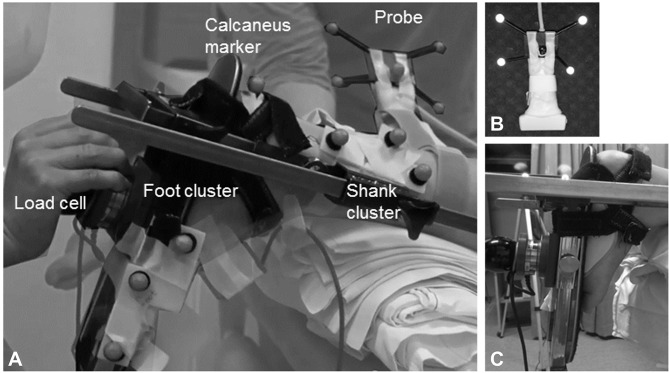
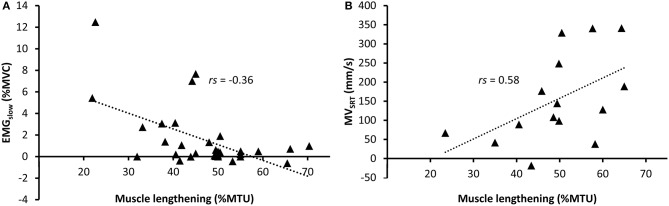
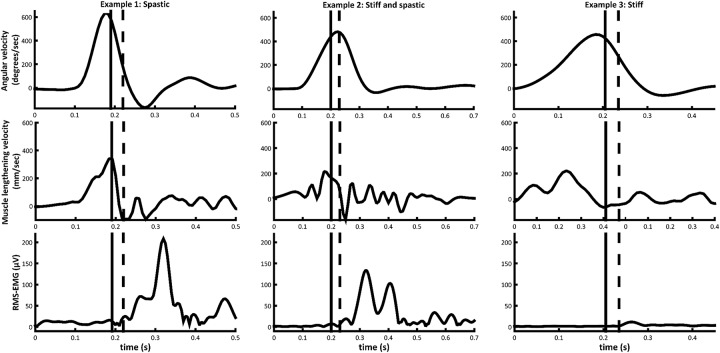
Stretch reflex hyperactivity in the gastrocnemius of children with spastic cerebral palsy (CP) is commonly evaluated by passively rotating the ankle joint into dorsiflexion at different velocities, such as applied in conventional clinical spasticity assessments. However, surface electromyography (sEMG) collected from the medial gastrocnemius (MG) during such examination reveals unexplained heterogeneity in muscle activation between patients. Recent literature also highlights altered muscle tensile behavior in children with spastic CP. We aimed to document MG muscle and tendon lengthening during passive ankle motion at slow and fast velocity and explore its interdependence with the elicited hyperactive stretch reflex. The ankle of 15 children with CP (11 ± 3 years, GMFCS 9I 6II, 8 bilateral, 7 unilateral) and 16 typically developing children (TDC) was passively rotated over its full range of motion at slow and fast velocity. Ultrasound, synchronized with motion-analysis, was used to track the movement of the MG muscle-tendon junction and extract the relative lengthening of muscle and tendon during joint rotation. Simultaneously, MG sEMG was measured. Outcome parameters included the angular and muscle lengthening velocities 30 ms before EMG onset and the gain in root mean square EMG during stretch, as a measure of stretch reflex activity. Compared to slow rotation, the muscle lengthened less and stretch reflex activity was higher during fast rotation. These velocity-induced changes were more marked in CP compared to TDC. In the CP group, muscle-lengthening velocity had higher correlation coefficients with stretch reflex hyperactivity than joint angular velocity. Muscles with greater relative muscle lengthening during slow rotation had earlier and stronger stretch reflexes during fast rotation. These initial results suggest that ankle angular velocity is not representative of MG muscle lengthening velocity and is less related to stretch reflex hyperactivity than MG muscle lengthening. In addition, muscles that lengthened more during slow joint rotation were more likely to show a velocity-dependent stretch reflex. This interdependence of muscle lengthening and stretch reflexes may be important to consider when administering treatment. However, muscle and tendon lengthening properties alone could not fully explain the variability in stretch reflexes, indicating that other factors should also be investigated.
Keywords: EMG; cerebral palsy; dynamic ultrasound; medial gastrocnemius; muscle stiffness; spasticity; stretch reflexes.
Figures
Similar articles
-
The relation between spasticity and muscle behavior during the swing phase of gait in children with cerebral palsy.Res Dev Disabil. 2014 Dec;35(12):3354-64. doi: 10.1016/j.ridd.2014.07.053. Epub 2014 Sep 18. Res Dev Disabil. 2014. PMID: 25240217
-
Muscle and tendon lengthening behaviour of the medial gastrocnemius during ankle joint rotation in children with cerebral palsy.Exp Physiol. 2018 Oct;103(10):1367-1376. doi: 10.1113/EP087053. Epub 2018 Sep 13. Exp Physiol. 2018. PMID: 30091806
-
Joint and Muscle Assessments of the Separate Effects of Botulinum NeuroToxin-A and Lower-Leg Casting in Children With Cerebral Palsy.Front Neurol. 2020 Apr 21;11:210. doi: 10.3389/fneur.2020.00210. eCollection 2020. Front Neurol. 2020. PMID: 32373040 Free PMC article.
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
Traumatic Brain Injury (TBI)-Induced Spasticity: Neurobiology, Treatment, and Rehabilitation.In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 14. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 14. PMID: 26269896 Free Books & Documents. Review.
Cited by
-
Comparing the Accuracy of Visual and Computerized Onset Detection Methods on Simulated Electromyography Signals with Varying Signal-to-Noise Ratios.J Funct Morphol Kinesiol. 2021 Aug 23;6(3):70. doi: 10.3390/jfmk6030070. J Funct Morphol Kinesiol. 2021. PMID: 34449669 Free PMC article.
-
Increased Ankle Plantar Flexor Stiffness Is Associated With Reduced Mechanical Response to Stretch in Adults With CP.Front Bioeng Biotechnol. 2021 Mar 25;9:604071. doi: 10.3389/fbioe.2021.604071. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 33842442 Free PMC article.
-
Muscle fascicle length adaptations to high-velocity training in young adults with cerebral palsy.Front Sports Act Living. 2025 May 13;7:1558784. doi: 10.3389/fspor.2025.1558784. eCollection 2025. Front Sports Act Living. 2025. PMID: 40433561 Free PMC article.
-
Stretching Interventions in Children With Cerebral Palsy: Why Are They Ineffective in Improving Muscle Function and How Can We Better Their Outcome?Front Physiol. 2020 Feb 21;11:131. doi: 10.3389/fphys.2020.00131. eCollection 2020. Front Physiol. 2020. PMID: 32153428 Free PMC article. Review.
-
Acute Effects of Static and Proprioceptive Neuromuscular Facilitation Stretching of the Plantar Flexors on Ankle Range of Motion and Muscle-Tendon Behavior in Children with Spastic Cerebral Palsy-A Randomized Clinical Trial.Int J Environ Res Public Health. 2022 Sep 15;19(18):11599. doi: 10.3390/ijerph191811599. Int J Environ Res Public Health. 2022. PMID: 36141875 Free PMC article. Clinical Trial.
References
-
- Lance J. Symposium Synopsis. In: E. Feldman RG, Young RR, Koella WP. editors. Spasticity: Disordered Motor Control. Chicago: Yearbook medical; (1980). p. 485–494.
-
- Gage JR. The Identification and Treatment of Gait Problems in Cerebral Palsy. 2nd ed. London: Mac Keith Press; (2009).
LinkOut - more resources
Full Text Sources
Miscellaneous