

Patterns of medication adherence in a multi-ethnic cohort of prevalent statin users diagnosed with breast, prostate, or colorectal cancer
- PMID: 30338462
- PMCID: PMC6238633
- DOI: 10.1007/s11764-018-0716-6
Patterns of medication adherence in a multi-ethnic cohort of prevalent statin users diagnosed with breast, prostate, or colorectal cancer
Abstract
Purpose: To investigate the implications of a cancer diagnosis on medication adherence for pre-existing comorbid conditions, we explored statin adherence patterns prior to and following a new diagnosis of breast, colorectal, or prostate cancer among a multi-ethnic cohort.
Methods: We identified adults enrolled at Kaiser Permanente Northern California who were prevalent statin medication users, newly diagnosed with breast, colorectal, or prostate cancer between 2000 and 2012. Statin adherence was measured using the proportion of days covered (PDC) during the 2-year pre-cancer diagnosis and the 2-year post-cancer diagnosis. Adherence patterns were assessed using generalized estimating equations, for all cancers combined and stratified by cancer type and race/ethnicity, adjusted for demographic, clinical, and tumor characteristics.
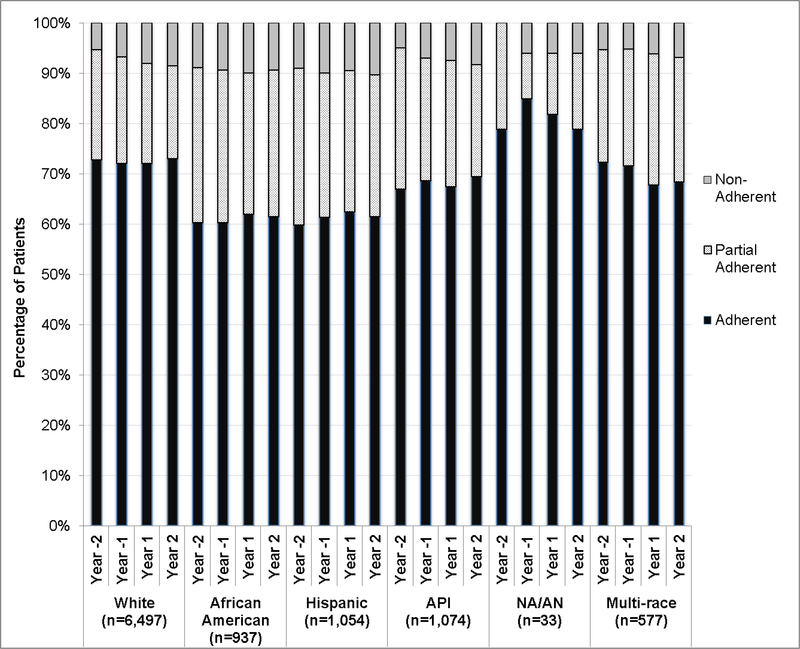
Results: Among 10,177 cancer patients, statin adherence decreased from pre- to post-cancer diagnosis (adjusted odds ratio (ORadj):0.91, 95% confidence interval (95% CI):0.88-0.94). Statin adherence decreased from pre- to post-cancer diagnosis among breast (ORadj:0.94, 95% CI:0.90-0.99) and colorectal (ORadj:0.79, 95% CI:0.74-0.85) cancer patients. No difference in adherence was observed among prostate cancer patients (ORadj:1.01, 95% CI:0.97-1.05). Prior to cancer diagnosis, adherence to statins was generally higher among non-Hispanic whites and multi-race patients than other groups. However, statin adherence after diagnosis decreased only among these two populations (ORadj:0.85, 95% CI:0.85-0.92 and ORadj:0.86, 95% CI:0.76-0.97), respectively.
Conclusions: We found substantial variation in statin medication adherence following diagnosis by cancer type and race/ethnicity among a large cohort of prevalent statin users in an integrated health care setting.
Implications for cancer survivors: Improving our understanding of comorbidity management and polypharmacy across diverse cancer patient populations is warranted to develop tailored interventions that improve medication adherence and reduce disparities in health outcomes.
Keywords: Adherence; Breast cancer; Colorectal cancer; Comorbidities; Prostate cancer; Race/ethnicity.
Figures
References
-
- American Cancer Society, Cancer Facts & Figures 2018. 2018, American Cancer Society: Atlanta, GA.
-
- Hilmer SN, et al. , A drug burden index to define the functional burden of medications in older people. Arch Intern Med, 2007. 167(8): p. 781–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
